by GAtherton
Last reviewed: April 2026…
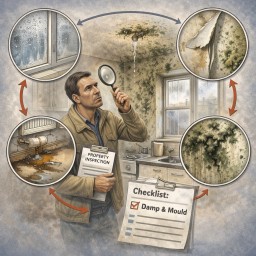
Date of check 4 March 2026 🆕…
Home › Knowledge Hub ›…
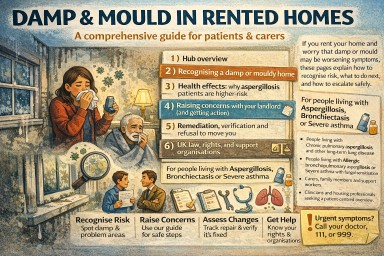
This page summarises key UK…