Antifungals
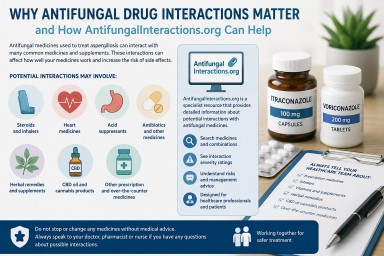

AntifungalInteractions.org – A Specialist Resource for Safer Antifungal Treatment
Last reviewed: April 2026…

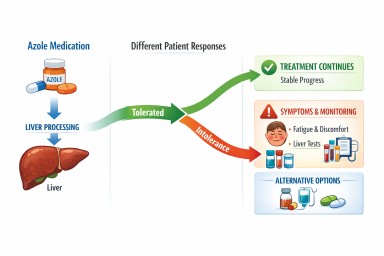
Antifungal drug interactions: what patients with aspergillosis need to know
Last reviewed: April 2026…
Last reviewed: April 2026…
Last reviewed: April 2026…