Living with Aspergillosis


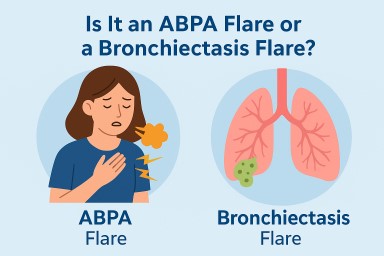
🫁 Is It an ABPA Flare or a Bronchiectasis Flare? How to Tell the Difference
If you have aspergillosis,…



🫁 Mucus Plugging in Aspergillosis: What It Is, Why It Happens, and What It Means
For patients with ABPA, CPA,…
If you have aspergillosis,…
For patients with ABPA, CPA,…