Browse information
Latest Articles
Support
For Professionals
Search
Lifestyle & Coping
Home
Living with Aspergillosis
Archive by Category "Lifestyle & Coping"
(
Page 2
)
Lifestyle & Coping
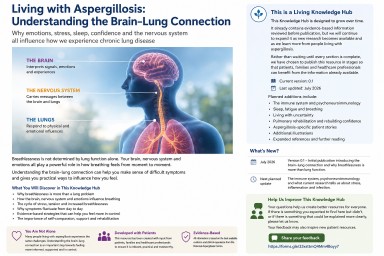
Living with Aspergillosis: Understanding the Brain–Lung Connection
by GAtherton
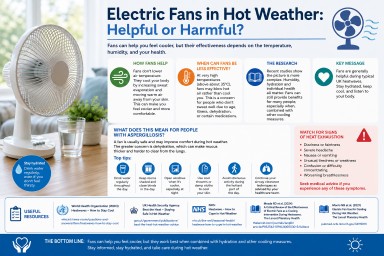
Electric Fans in Hot Weather: Helpful or Harmful?
by GAtherton
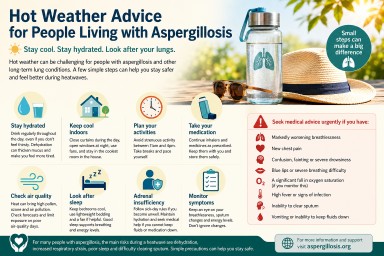
Hot Weather Advice for People Living with Aspergillosis
by GAtherton
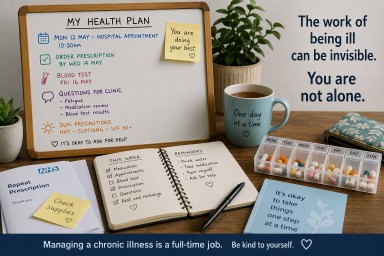
The Hidden Job Nobody Talks About: Living with Chronic Illness
by GAtherton
Living Safely with Pets When You Have Aspergillosis
by GAtherton
Healthy Eating Should Not Feel Like Punishment
by GAtherton
The Power of Keeping a Health Diary When You Have Aspergillosis
by GAtherton
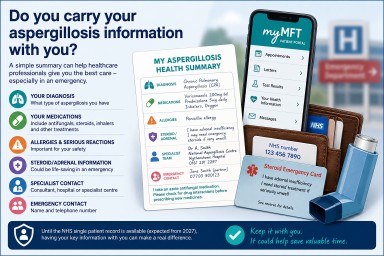
Do You Carry Your Aspergillosis Information With You?
by GAtherton
Exercise and Aspergillosis: How Physical Activity Can Improve Breathing, Strength and Wellbeing
Last reviewed: June 2026 Key…
by GAtherton
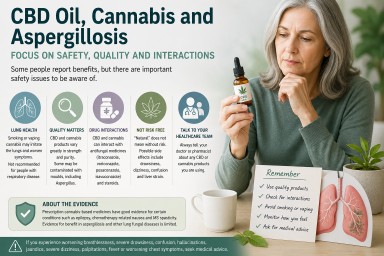
CBD Oil, Cannabis and Aspergillosis: Safety, Quality and Drug Interactions
by GAtherton
1
2
3
4
…
16