Steroid Use and Your Eyesight: What Patients Need to Know
Steroids (such as prednisolone, inhaled corticosteroids, eye drops, or steroid injections) are important medicines for conditions like asthma, allergic bronchopulmonary aspergillosis (ABPA), and other inflammatory illnesses. But they can also affect your eyesight — sometimes in subtle ways day-to-day, and sometimes with long-term risks.
This guide explains what may happen, why vision can fluctuate, and what you can do to protect your eyes.
How steroids can affect the eyes
-
Cataracts
Long-term steroids may cause a type of cataract at the back of the lens (posterior subcapsular). This can cause glare, blurred vision, or difficulty seeing in bright light. -
Glaucoma (raised eye pressure)
Steroids can increase pressure inside the eye, potentially damaging the optic nerve if untreated. This is more common with steroid eye drops, but tablets and inhalers can also contribute. -
Central Serous Retinopathy (CSR)
Fluid may build up under the retina, causing blurred or distorted central vision. Usually reversible when steroids are reduced or stopped, but it can recur. -
Blood sugar and fluid changes
Steroids raise blood sugar and shift body fluids. This can temporarily alter the eye lens, making vision sharper one day and blurrier the next. -
Delayed healing and infection risk
Steroids can make eye infections worse or delay healing after injury or surgery.
Why vision changes from day to day
Some patients notice that their glasses seem to “work” differently depending on their steroid dose. Reasons include:
-
Time of day: Vision may blur a few hours after taking a dose, when steroid levels peak.
-
Dose level: Higher doses cause more fluctuation; tapering can also make vision variable.
-
Delivery method:
-
Tablets: most likely to cause daily swings.
-
Eye drops: may raise eye pressure within hours.
-
Inhalers: usually small risk, unless high dose over many years.
-
-
Other factors in asthma/aspergillosis: Nebulisers, oxygen, antifungal medicines (like voriconazole), fatigue, and infections can all add to vision changes.
What patients can do
Day-to-day management
-
Drink plenty of water to help with fluid balance.
-
Eat regularly and limit sugary snacks to reduce blood sugar swings.
-
Use good lighting and take regular breaks from close work.
-
Try to take steroids at the same time each day for more predictable effects.
-
Keep a diary of when blurred vision happens in relation to your dose.
Eye care
-
Tell your optician and GP you are on long-term steroids.
-
Ask for regular eye checks (pressure and cataract screening every 6–12 months).
-
Don’t rush to buy new glasses if your prescription seems to keep changing — vision often settles once steroid doses stabilise.
-
Lubricating eye drops can help if dryness is a problem.
When to seek urgent help
-
Sudden or severe blurred vision
-
Dark spots, flashing lights, or distorted shapes
-
Eye pain, halos around lights, or redness
-
Rapid worsening of eyesight
These could be signs of glaucoma, cataract progression, or retinal changes and need prompt medical attention.
Key message
Not everyone on steroids will notice eyesight problems, but it is a well-recognised side effect. The changes are often temporary and reversible, especially the day-to-day fluctuations, but long-term use does carry risks.
By being aware, monitoring regularly, and working with both your doctor and optician, you can catch problems early and protect your sight.
Integrated Care Boards (ICBs): What They Are and How Patients Can Contact Them

What is an ICB?
-
An Integrated Care Board (ICB) is the NHS organisation that replaced Clinical Commissioning Groups (CCGs) in July 2022.
-
Each ICB plans and funds NHS services across a large region (1–3 million people).
-
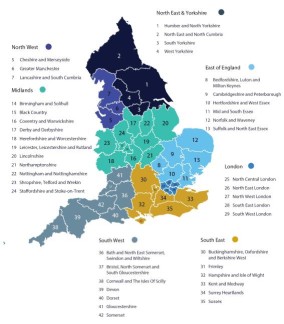
England has 42 ICBs, covering the whole country (see full list plus contact details here).
-
They hold the NHS budget locally, decide which services are provided, and work with councils and community organisations.
- Scotland, Wales and Northern Ireland have a different system
Why might a patient need to contact an ICB?
Patients don’t normally deal with ICBs day-to-day (you’ll usually go to your GP, hospital, or local Patient Advice and Liaison Service). But there are situations where you may want or need to reach out:
-
Feedback or complaints about NHS services that can’t be resolved at GP or hospital level.
-
Service changes – ICBs must consult the public when they change how services are delivered (e.g. reorganising clinics, closing or merging hospital departments).
-
Patient voice – ICBs have teams dedicated to patient and public involvement. You can join forums, respond to surveys, or attend public meetings.
-
Access to care – if you are struggling to access a specialist service or want to know what’s available in your area, ICBs can advise.
-
Equality of access – raising concerns if a particular group or community is being left behind.
How can a patient contact an ICB?
-
Patient Experience / Engagement Teams: Every ICB has an email and phone number for patients. Look for “Get Involved” or “Contact Us” on their website.
-
PALS escalation: If PALS (Patient Advice and Liaison Service) can’t resolve your concern, they can refer it up to the ICB.
-
Public board meetings: ICBs must hold regular meetings in public where patients can submit questions.
-
Healthwatch: Your local Healthwatch can raise issues directly with the ICB on your behalf.
✅ In summary:
Patients usually don’t need to contact an ICB for routine issues, but if you want your voice heard about service changes, access problems, or unresolved complaints, the ICB is the organisation responsible for commissioning services in your area.

Comparing Health Systems: NHS vs Insurance-Based Models

Healthcare looks very different depending on where you live, and it can be informative to look at the pros and cons of each system.
The UK’s NHS model is often contrasted with insurance-based systems such as those in the US and Germany. All aim to look after patients, but they differ in cost, access, caution with new medicines, and their contribution to research.
1. Funding and Access
NHS (UK)
-
Publicly funded through taxation.
-
Care is free at the point of use.
-
Limited co-payments (e.g. prescriptions in England, but free in Scotland/Wales/NI).
Insurance-Based (US, Germany)
-
US: Mix of private insurance, employer-based plans, and public programs (Medicare/Medicaid). Patients often pay premiums, deductibles, and co-pays.
-
Germany: Statutory health insurance (public) plus private options. Patients contribute through payroll and some co-payments.
✅ Equity difference: The NHS ensures universal coverage. Insurance systems can create gaps — in the US, uninsured or underinsured patients face very high bills.
2. Cost
-
United States: ~16–17% of GDP, >$12,000 per person per year.
-
Germany: ~11–12% of GDP, ~$6,000–7,000 per person.
-
United Kingdom: ~10% of GDP, ~$4,500 per person.
✅ Insurance-based systems are much more expensive overall. The NHS achieves lower cost per head but sometimes with tighter rationing.
3. Approach to New Medicines
NHS (cautious, evidence-driven)
-
Drugs are appraised by NICE (National Institute for Health and Care Excellence).
-
Only those proven clinically effective and cost-effective are routinely available.
-
Access can be slower, but ensures sustainability and safety.
Insurance-Based (faster, autonomy-driven)
-
Once a drug is licensed (FDA in US, EMA in EU), doctors may prescribe it, often off-label.
-
Patients may be offered newer or experimental options earlier.
-
Shared decision-making: “This might help, here are the risks, do you want to try it?”
✅ Trade-off: Insurance systems offer earlier access, but higher risk of side effects, wasted cost, and overuse. NHS offers more consistency but less flexibility.
4. Risks of Wide Access
Allowing rapid use of new drugs can lead to:
-
Harm to patients:
-
US:
-
Vioxx (rofecoxib) was widely prescribed for arthritis before long-term data was available → later linked to tens of thousands of excess heart attacks and strokes.
-
Opioid overprescribing (encouraged by drug companies, reimbursed by insurers) fuelled a public health crisis, with millions addicted and >500,000 deaths.
-
-
Germany: Wider acceptance of MCAS and other “working diagnoses” sometimes leads to long-term medication without solid evidence, exposing patients to risks without clear benefit.
-
-
Harm from NHS caution:
-
UK:
-
Cystic fibrosis drug Orkambi: available in the US and Germany years earlier, but withheld in the UK until 2019 due to cost-effectiveness debate → children and young adults missed out on years of treatment.
-
Cancer immunotherapies: delays in NICE approval have meant some patients only got access through special trials or not at all, potentially shortening survival.
-
-
5. Doctor–Patient Conversations
-
Insurance systems: “You may have this condition, and drug X or Y might help. It’s your choice.”
-
NHS: “We know you have this condition. X is proven and available. Y is unproven or not funded, so we cannot recommend it.”
✅ Insurance systems emphasise autonomy and options. The NHS emphasises evidence and fairness.
6. UK Private Healthcare vs US Healthcare
It’s tempting to think the UK private sector is equivalent to the US system, but they are very different.
UK Private Care
-
Covers about 10–12% of the population, mainly for elective surgery, scans, and faster consultant appointments.
-
Usually funded by employer insurance or self-pay.
-
Still relies on the NHS for emergencies and complex care.
-
New medicines still follow NICE approval — patients don’t usually get earlier access to unapproved drugs.
US Healthcare
-
Insurance-based and the default system, covering almost everyone.
-
Patients pay premiums, deductibles, and co-pays — bills can be catastrophic without good cover.
-
Emergencies are treated but still billed.
-
Patients may access new drugs and technology earlier, but often at very high cost.
✅ Bottom line: UK private care is an add-on to the NHS, giving faster access but within the same medical framework. The US system is entirely insurance-driven, with no NHS-style universal fallback.
7. Research Strengths
-
Insurance-based systems (esp. US):
-
Huge budgets (NIH + pharma).
-
Early adoption → more real-world data.
-
Specialist centres attract rare-disease patients.
-
-
NHS system:
-
Unified data across the whole population.
-
Ability to run massive pragmatic trials cheaply (e.g. RECOVERY during COVID: identified dexamethasone as life-saving within weeks).
-
More representative recruitment because care is universal.
-
✅ Together they complement each other:
-
New drugs are often developed and trialled first in the US/Germany.
-
Large-scale validation and population-level studies often happen in the UK.
8. Which System Is “Better”?
It depends what you value most:
-
Insurance-based systems:
-
More expensive
-
Faster access to innovation
-
More choice and autonomy
-
Higher risk of harm and inequality
-
-
NHS:
-
Less expensive
-
Slower, more cautious
-
Equitable and universal
-
Sometimes frustratingly restrictive
-
✅ Bottom Line
No system is perfect.
-
Insurance-based systems favour speed, choice, and innovation — but have caused harm through early adoption of unsafe drugs, opioid overuse, and inequitable access.
-
The NHS favours equity, safety, and sustainability — but has harmed patients by delaying access to life-saving treatments while cost-effectiveness was debated.
-
UK private healthcare is not a parallel US-style system: it is simply a faster lane within the NHS framework, not an alternative to universal coverage.
The reality is that both types of systems need each other: innovations often emerge in the US/Germany, while the NHS provides the gold standard for large-scale testing and equitable delivery.
Mast Cell Activation Syndrome (MCAS), Mastocytosis, and Aspergillosis: What Patients Need to Know
What is MCAS?
Mast cells are immune cells that release chemicals like histamine to fight infection and respond to allergens. In Mast Cell Activation Syndrome (MCAS), mast cells release their chemicals too easily or too often.
This can cause a wide range of allergy-like symptoms, including:
-
Flushing, itching, hives
-
Wheezing or chest tightness
-
Abdominal pain, diarrhoea, nausea
-
Drop in blood pressure, dizziness, “anaphylaxis-like” episodes
-
Fatigue and brain fog
Unlike systemic mastocytosis (see below), in MCAS the number of mast cells is normal — they are just overactive.
What is Mastocytosis?
Mastocytosis is a rare disease where the body makes too many mast cells, which then build up in the skin, bone marrow, or other organs.
-
Symptoms can include skin spots (urticaria pigmentosa), itching, flushing, abdominal pain, or even severe allergic reactions.
-
It is usually diagnosed with a bone marrow biopsy, persistently raised tryptase levels, and sometimes genetic testing (KIT mutations).
-
It is much rarer than MCAS — affecting perhaps 1 in 10,000–20,000 people.
-
Unlike MCAS, it is well-recognised by the NHS and has clearer diagnostic criteria.
👉 Key difference:
-
Mastocytosis = too many mast cells (rare, testable, well-defined).
-
MCAS = mast cells behaving abnormally (more common, debated, less defined).
Why is MCAS controversial?
The problem is not whether patients are unwell — their symptoms are very real. The debate is about diagnosis:
-
No gold-standard test: mast cell markers (tryptase, histamine, prostaglandins) fluctuate, so results may be normal between flares.
-
Overlapping symptoms: MCAS can look like asthma, ABPA, IBS, coeliac disease, POTS, autoimmune disease, or anxiety.
-
Different acceptance worldwide: in the US and Germany, MCAS is more widely recognised; in the NHS, it is rarely diagnosed formally.
-
Risk of mislabelling: some doctors fear that calling everything “MCAS” could delay other correct diagnoses.
MCAS is still being debated and developed
It is important to understand that MCAS is a work in progress:
-
International allergy bodies (AAAAI, EAACI, WAO) are actively developing clearer diagnostic criteria.
-
Research is ongoing into more reliable biomarkers (tryptase, histamine metabolites, prostaglandin D2) and genetic links.
-
Different schools of thought: some specialists see MCAS as common and under-recognised, others worry about overdiagnosis.
-
NHS position: the UK is cautious, waiting for stronger evidence before making MCAS a routine diagnosis.
-
Future direction: most experts expect MCAS will eventually be better defined, possibly with subtypes (allergic, autoimmune, idiopathic), clearer tests, and tailored treatments such as biologics.
👉 For now, patients should know: MCAS is real for many, but it remains under scientific development, which is why experiences differ depending on which doctor you see.
MCAS and Aspergillosis – is there a link?
There is no proven direct link between MCAS and aspergillosis, but there are overlaps:
-
In Allergic Bronchopulmonary Aspergillosis (ABPA), mast cells release histamine and other mediators in response to Aspergillus spores — very similar to MCAS.
-
In Chronic Pulmonary Aspergillosis (CPA), mast cells are found in lung tissue, but their role isn’t well understood.
-
Both conditions can cause wheeze, fatigue, breathlessness, and allergic-type symptoms, though for different reasons.
Some specialists suggest patients with very sensitive mast cells may react more strongly to fungal exposure. Conversely, chronic fungal inflammation may “prime” mast cells to overreact.
Why careful diagnosis matters
It’s possible to see a patient who looks like they have MCAS but actually responds to another diagnosis and treatment:
-
Asthma/ABPA → inhaled steroids, biologics, antifungals
-
POTS → fluids, salt, and blood-pressure medicines
-
Coeliac disease/IBS → dietary management
-
Autoimmune disease → immunosuppressants
This is why doctors are cautious: assuming MCAS too quickly could delay the right treatment.
What the future may hold
-
Better definitions: international allergy societies are working on clearer criteria to separate MCAS from other conditions.
-
More research: scientists are studying mast cell biology, genetics, and biomarkers.
-
Improved treatments: antihistamines, mast cell stabilisers, and leukotriene blockers are already used; biologics (like omalizumab or dupilumab) are being studied.
-
Greater NHS recognition: if stronger evidence emerges, MCAS is more likely to be formally recognised in the UK.
Differences between countries
-
In the US and Germany, MCAS is more widely recognised, and patients may find it easier to get the label and access to mast-cell–targeted treatments (antihistamines, leukotriene blockers, mast cell stabilisers, biologics in some cases).
-
In the UK/NHS, doctors are much more cautious and rarely use “MCAS” as a formal diagnosis, even when symptoms fit. Treatment is often offered pragmatically, without the label.
-
Does this mean outcomes are better in the US/Germany?
-
There is no strong evidence yet that patients in those countries do better long-term just because they get the MCAS diagnosis.
-
What’s different is mostly access to recognition and treatment, not proven improvements in quality of life compared with the UK.
-
Ongoing research is needed to show whether having the diagnosis itself improves patient outcomes.
-
Key take-home message for aspergillosis patients
-
MCAS is real for patients, but controversial in medicine. The debate is about safe diagnosis, not whether people are genuinely unwell.
-
Mastocytosis is different: it is rare, clearly defined, and testable — whereas MCAS is more common but less well recognised.
-
Aspergillosis overlaps with MCAS because both involve mast cell activity and histamine release, especially in ABPA.
-
Different countries handle it differently: US/Germany diagnose it more often, the UK is cautious — but there is no clear proof yet that outcomes are better where it’s recognised more widely.
-
The most important thing is to get a careful, accurate diagnosis, so the right treatment can be given — whether that turns out to be MCAS, asthma, ABPA, or another condition.
👉 In short: Mastocytosis is rare and well-defined. MCAS is more common but debated. Both share features with aspergillosis, especially ABPA. MCAS is still being researched and developed, and while some countries recognise it more widely, there’s no solid evidence yet that this leads to better outcomes than the cautious UK approach.

Personality, Connection, and Mental Health

Everyone has different ways of keeping emotionally balanced. Some people need lots of contact with others, while some need quiet time to recharge. Others feel best when they mix both. Recognising your “type” isn’t about putting yourself in a box — it’s about understanding what you need to stay well.
1. The Connector
-
How they thrive: by spending time with friends, family, or groups.
-
Mental health benefit: being around others boosts mood, reduces anxiety, and gives a sense of belonging.
-
Challenges: isolation or long stretches without company can lead to loneliness, low mood, or feeling cut off.
-
Helpful strategies:
-
Build regular contact into your week (calls, visits, online groups).
-
Explain to family/friends that contact isn’t a “nice extra” but an essential for your wellbeing.
-
Use support groups (like NAC CARES) to stay connected if health limits travel.
-
2. The Reflector
-
How they thrive: by having quiet, personal space to recharge after socialising.
-
Mental health benefit: time alone helps calm the nervous system, reduce stress, and spark creativity.
-
Challenges: may feel drained if pressured into constant social contact. Can appear “distant” to others when actually just recharging.
-
Helpful strategies:
-
Protect quiet time without guilt — see it as fuel, not selfishness.
-
Use calming practices (journaling, meditation, walks, hobbies).
-
Communicate with loved ones: “I need some downtime, then I’ll rejoin.”
-
3. The Balancer
-
How they thrive: with a healthy mix of both social contact and private time.
-
Mental health benefit: balance allows them to enjoy connection without becoming overstimulated.
-
Challenges: may tip too far one way — overbooking social time and burning out, or retreating too much and feeling lonely.
-
Helpful strategies:
-
Notice your signals — irritability might mean you need rest, loneliness means you need contact.
-
Plan weeks with both connection (calls, visits) and rest (quiet evenings, gentle hobbies).
-
4. The Helper
-
How they thrive: by supporting and caring for others. Helping gives meaning and boosts self-worth.
-
Mental health benefit: gives purpose and strengthens relationships.
-
Challenges: may neglect their own needs, leading to burnout or resentment.
-
Helpful strategies:
-
Follow the “oxygen mask rule” — you can only help others if you look after yourself.
-
Schedule self-care alongside care for others.
-
Accept help when offered — balance is key.
-
5. The Explorer
-
How they thrive: through novelty, discovery, and learning. They love trying new things, meeting new people, or exploring new ideas.
-
Mental health benefit: curiosity and new experiences can reduce boredom, lift mood, and spark resilience.
-
Challenges: chronic illness can limit physical adventures, which may feel like a loss of identity.
-
Helpful strategies:
-
Adapt “exploring” to your situation — online learning, virtual tours, new books or creative hobbies.
-
Set small, achievable challenges so you still get a sense of growth.
-
Why this matters for mental health
-
There is no “right” type. Each way of recharging is valid. Problems arise when we don’t recognise or honour our needs.
-
Stress comes when needs aren’t met. A Connector without contact feels lonely; a Reflector without quiet feels overwhelmed.
-
Self-awareness protects wellbeing. Knowing your type helps you explain your needs to family, friends, and even your healthcare team.
Key message for aspergillosis patients
Chronic illness can magnify these needs. Fatigue, isolation, or hospital visits may disrupt your usual coping style. Recognising whether you’re a Connector, Reflector, Balancer, Helper, or Explorer can guide you to the right kinds of support.
👉 In short: protect what restores you. Whether it’s people, quiet, balance, helping, or exploring, these are not luxuries — they are the building blocks of good mental health.

Grief and the Loss of Health in Aspergillosis
Understanding grief
Grief is usually thought of as the response to the death of a loved one, but it is more than that. Grief is the natural human reaction to any major loss — whether of a person, a role, a relationship, or one’s health.
For people living with aspergillosis, grief often arises not only from bereavement but also from the daily reality of lost health, independence, and certainty about the future. This type of grief is sometimes overlooked by others, yet it is just as valid and just as painful.
Bereavement grief vs. health-related grief
Grieving a loved one
When a person we love dies, the grief process involves:
-
Remembering and honouring the relationship.
-
Finding ways to carry that memory forward through photos, anniversaries, stories, or rituals.
-
Adjusting to life in their absence while keeping a continuing bond.
The work of bereavement grief is therefore about preserving connection to memory and integrating loss into our life story.
Grieving health
By contrast, grieving the loss of health is about adapting to change in the present and future:
-
Our body no longer works as it once did.
-
Activities and roles that defined us may no longer be possible.
-
Identity and self-image shift as illness reshapes daily life.
The task here is not to “hold on” to a memory, but to rebuild life around a new reality. Patients often grieve the loss of their “old self” — the person who could climb stairs, walk long distances, work, or join in family activities without limitation.
👉 Put simply:
-
Bereavement grief = finding ways to remember.
-
Health-related grief = finding ways to adapt.
Why health loss grief is particularly difficult
For people with aspergillosis (and other long-term conditions), this grief is uniquely challenging because:
-
The loss is ongoing – illness can fluctuate, relapse, or progress, so grief is re-triggered many times.
-
It is invisible – others may not see how devastating the loss of health feels, which adds loneliness.
-
It is about the self – we mourn not just someone else but the person we used to be.
-
It holds uncertainty – unlike death, health loss sits in a space between grief and hope, as treatments may stabilise or improve things, but may not restore the past.
How to adapt and live with health-related grief
1. Recognise it for what it is
-
Naming these feelings as grief helps reduce guilt and self-blame. You are not “weak” or “failing” — you are adjusting to a major life change.
2. Give space for feelings
-
Sadness, anger, frustration, and even envy are normal. Suppressing them often prolongs the pain.
3. Use safe outlets
-
Talk with others who understand — family, friends, support groups, or counsellors.
-
Write in a journal, make art, or use rituals (like lighting a candle or planting a tree) to symbolise change.
4. Maintain connection and meaning
-
Illness may limit old roles, but it does not erase identity. People often rediscover purpose through hobbies, creativity, peer support, or volunteering.
5. Focus on what’s possible now
-
Set small, realistic goals — e.g. walking to the garden, preparing a simple meal, joining a call.
-
Celebrate these achievements, rather than only comparing yourself to your old abilities.
6. Care for your body
-
Sleep, nutrition, and gentle movement (as tolerated) improve energy and resilience.
7. Seek professional support if needed
-
If grief leads to ongoing despair, anxiety, or hopelessness, ask your GP about counselling or NHS Talking Therapies. Support is available, and you don’t have to carry this alone.
Resources
UK-based
-
NHS Talking Therapies – free counselling/CBT for anxiety and depression.
-
MIND – support for mental health and loss.
-
Asthma + Lung UK – helpline and groups for lung disease.
-
Cruse Bereavement Support – guidance on grief that can apply to non-death losses.
-
NAC CARES (aspergillosis.org) – patient meetings, forums, and tailored educational resources.
International / Online
-
What’s Your Grief – blogs, courses, and podcasts on different types of grief.
-
The Mighty – online community sharing experiences of chronic illness and loss.
Books
-
How to Live Well with Chronic Pain and Illness – Toni Bernhard.
-
When the Body Says No – Gabor Maté.
-
On Grief and Grieving – Elisabeth Kübler-Ross & David Kessler.
Videos
-
Grieving with a Chronic Illness (YouTube).
-
Living with Loss: Navigating Grief in Chronic Illness (YouTube).
-
Letting Go of Grief and Guilt with Chronic Illness (YouTube).
Final message for patients
Grief from health loss is real, human, and normal. It is not about weakness, nor about giving up. It is about learning how to live differently — with compassion for yourself, space for your feelings, and courage to rebuild purpose in new ways.
While bereavement grief holds on to memory, health grief asks us to adapt. Both are valid, both are painful, and both can soften with time, support, and self-kindness.
👉 You are not alone — others with aspergillosis and chronic illness are walking the same path, and support is out there to help you carry it. 💙

Mannose-Binding Lectin (MBL) Deficiency and Aspergillosis
What is MBL?
Mannose-binding lectin (MBL) is a natural protein made by the immune system. Its job is to help the body recognise and fight off germs, including fungi like Aspergillus. It’s part of the “innate” immune system – the first line of defence you’re born with.
How common is MBL deficiency?
MBL deficiency is surprisingly common.
-
Around 5–10% of people have very low or absent levels.
-
If you include milder reductions, as many as 20–30% of people carry genetic changes that lower MBL activity.
For most, this causes no problems because the immune system has other pathways to fall back on. People often never know they have it.
Why do MBL levels vary?
-
Genetics: The MBL2 gene comes in different versions, some producing plenty of MBL and others producing little or none.
-
Inheritance: The combination of gene copies from each parent determines your level.
-
Normal diversity: Low levels are common and often harmless, showing the immune system has strong backup pathways.
Are some people born more vulnerable to infection?
Yes – but it depends on the situation.
-
Children with very low MBL may get more ear, chest, or sinus infections while their immune systems are developing.
-
In adults, MBL deficiency usually only matters if there are other risks, such as chronic lung disease, immune suppression, or another immune problem.
-
Many people with low MBL live their whole lives without extra infections.
MBL deficiency and aspergillosis
On its own, MBL deficiency rarely causes illness. But in people who already have other risks – such as lung disease (COPD, asthma, bronchiectasis, or TB damage) or a weakened immune system – it may make infections more likely.
Research suggests MBL deficiency can be linked to:
-
Chronic pulmonary aspergillosis (CPA)
-
Allergic bronchopulmonary aspergillosis (ABPA)
-
Invasive aspergillosis in people with suppressed immunity
In these cases, MBL deficiency is not the single cause of aspergillosis, but it may be one of several factors that increase vulnerability.
Can MBL deficiency be treated?
At present, there is no routine treatment to replace MBL itself. Research has explored giving purified MBL, but it hasn’t become a standard therapy – largely because deficiency is so common and most people remain healthy without intervention.
Instead, management focuses on:
-
Treating infections promptly with antibiotics or antifungals
-
Sometimes using preventive (prophylactic) antibiotics or antifungals in people with frequent or severe infections
-
Using immunoglobulin replacement therapy if there are additional immune problems
-
Supporting lung health and reducing risks with vaccinations, good self-care, and specialist monitoring
Why measure MBL if it can’t be treated directly?
Even without a direct treatment, measuring MBL can still be useful:
-
Helps explain recurrent infections – finding a low MBL level can give part of the reason why someone is more prone to infections.
-
Part of a bigger immune work-up – it’s often checked alongside other immune tests, and the overall pattern may guide treatment decisions.
-
Risk awareness – knowing about low MBL can make doctors more proactive with antibiotics, antifungals, or vaccinations, and encourage earlier treatment at the first sign of infection.
-
Research value – helps specialists understand why some people develop aspergillosis while others don’t.
Why hasn’t evolution eliminated low MBL?
-
Common worldwide: 5–10% of people have very little MBL, and up to 30% have reduced levels. If this were a major disadvantage, numbers would be lower.
-
Other immune pathways compensate: The body has strong backup systems, so many people stay healthy even with low MBL.
-
Possible advantage: In some infections, high MBL may drive too much inflammation. Lower MBL might have protected against diseases like leprosy or TB.
-
Changing disease patterns: In the past, people rarely lived long enough for chronic lung disease to show the effects of low MBL. Today, with longer lives and modern medicine, its role is more visible.
👉 In short: low MBL has not been “selected out” by evolution because it usually isn’t harmful on its own, and in some situations it may even have been protective.
What this means for patients
-
Having MBL deficiency is quite common and usually harmless.
-
It may become more relevant if you also have underlying lung disease or are on treatments that suppress the immune system.
-
If MBL deficiency is suspected, doctors may check for it as part of a wider immune work-up.
-
The key point: treatment is aimed at managing infections and lung health, not the MBL level itself.
👉 In short: MBL deficiency is common in the general population. Most people never notice it, but for some with lung disease or weakened immunity, it may add to the risk of aspergillosis. While there’s no direct treatment for the deficiency, testing can help explain recurrent infections, guide wider immune checks, and shape preventive care.

Autumn 2025 COVID-19 Booster – What Aspergillosis Patients Need to Know
The UK Health Security Agency (UKHSA) has updated who will be offered the COVID-19 booster this autumn. The programme is now more limited than in 2024, so it’s important to know if you qualify.
Who will be offered the booster?
You can get a free COVID-19 booster this autumn if you are:
-
Aged 75 or over
-
Living in a care home for older adults
-
Aged 6 months or older and immunosuppressed
This is a change from 2024, when everyone aged 65+ and many other clinical risk groups were included.
What “immunosuppressed” means
Many people with aspergillosis fall into this category. You may be considered immunosuppressed if you are:
-
Taking systemic steroids for more than a month
-
Receiving biologic therapy or other immunomodulatory medication
-
Living with a condition that affects your immune system
-
Having had chemotherapy, radiotherapy, or a transplant
If you’re unsure whether this applies to you, check with your GP or hospital specialist.
Timing of the booster
-
Boosters are usually offered at least 6 months after your last dose, including the spring booster.
-
Even if you’ve never had a COVID-19 vaccine before, you can still get one this autumn if you are in one of the eligible groups.
Why this matters for aspergillosis patients
People with aspergillosis often have weaker lungs and higher risks from infections. If your immune system is also suppressed by medication or illness, COVID-19 can be more severe. The booster offers added protection during the winter months.
💙 Key advice:
-
If you are immunosuppressed or over 75, you should be offered the vaccine.
-
If you think you qualify but haven’t received an invitation, speak to your GP or specialist.
-
Don’t delay — protecting yourself against COVID-19 is especially important when living with aspergillosis.
📌 Full details from UKHSA: Who’s eligible for the 2025 COVID-19 vaccine or autumn booster
Why the NHS doesn’t use unvalidated tests (and why that’s not just being awkward)
It can feel frustrating when the NHS won’t accept private tests like mycotoxin panels, IgG food intolerance kits, or home mould testing. But this isn’t about being difficult — it’s about protecting patients and making sure care is fair, safe, and effective.
-
Safety first
Unvalidated tests can give false positives (saying you have a problem when you don’t) or false negatives (missing something important). Acting on the wrong result could lead to unnecessary medication, restrictive diets, or missed diagnoses. -
Evidence matters
NHS doctors can only use tests that have been proven in research to give accurate, meaningful results. That way, they can be confident the result will actually help guide treatment. -
Protecting patients from harm
Many private tests are expensive and may push people toward costly supplements, detox regimes, or antifungals they don’t need. The NHS avoids recommending anything that risks harm or waste. -
Fairness and trust
The NHS has to provide care that is fair for everyone. That means sticking to tests and treatments that have passed strict checks for accuracy, safety, and usefulness.
💙 Key message: When the NHS says “we can’t use that test,” it’s not about being awkward or dismissive — it’s about making sure that what’s offered is safe, reliable, and genuinely helps patients.
Private companies that sell mycotoxin or food intolerance tests will naturally try to justify their services — it’s their business, after all. But before you spend money, it’s worth asking one key question: ‘Will my NHS doctor be able to use these results to guide my treatment?’ If the answer is no (and in most cases it is), then you may just be spending a lot of money without getting anything useful for your care.
That doesn’t mean your symptoms aren’t real — it just means these particular tests aren’t the right tool. NHS doctors can only act on validated results (like CT scans, Aspergillus antibody blood tests, or sputum cultures) because those are proven to be accurate and safe.

Inhaled Mycotoxins and Testing: What Patients Need to Know
Many patients ask about mould, mycotoxins, and private test panels — especially when symptoms overlap with conditions like aspergillosis, asthma, or MCAS (see glossary). The science is complex, and there’s a lot of misinformation online. Here’s what we know.
Can inhaled mycotoxins cause illness?
-
High exposure at work: In farming, animal feed, waste handling, or recycling, workers can breathe in dusts that contain fungal fragments and mycotoxins. At these levels, people may develop work-related asthma, cough, or “organic dust toxic syndrome.”
-
Homes and offices: Damp and mouldy buildings are consistently linked to worse asthma and respiratory symptoms. But experts (WHO, Institute of Medicine, CDC, MHRA) stress that it’s not just mycotoxins — spores, allergens, β-glucans, and bacteria all play a role.
-
Bottom line: Dampness and mould are unhealthy, but there’s limited proof that airborne mycotoxins alone at household levels cause chronic illness. The key intervention is always fixing damp and mould, improving ventilation, and managing lung conditions properly.
Why are private mycotoxin tests offered?
Despite the limited evidence, urine and blood “mycotoxin panels” are marketed by private labs (often in the US). They detect tiny traces of toxins that almost everyone has — mostly from food.
Why they exist:
-
People with real symptoms want answers, and commercial labs meet that demand.
-
It is technically possible to measure mycotoxins, even if the meaning is unclear.
-
Some alternative practitioners use them because patients want something tangible.
Why are these tests unreliable?
-
Everyone has some exposure – Sensitive tests will almost always find traces from normal diet, even in healthy people.
-
No agreed cut-offs – No international standards for what level in blood/urine is “safe” or “unsafe.”
-
Not validated for diagnosis – NHS, WHO, CDC, EMA do not accept these tests as diagnostic.
-
Can’t show source – They can’t distinguish whether the toxin came from food, dust, or infection.
-
Risk of unnecessary treatment – May push people toward costly, unproven therapies.
👉 Bottom line: A positive result usually reflects diet, not disease. That’s why NHS doctors don’t use these tests.
Why validation matters
For any medical test to be trusted, it must go through validation:
-
Analytical validation – does the test reliably measure what it claims?
-
Clinical validation – does it correctly identify people with the disease and exclude those without it?
-
Clinical utility – does it actually help doctors make better treatment decisions?
-
Regulatory approval – bodies like the MHRA (UK), FDA (US), and EMA (EU) ensure tests are safe and meaningful before routine use.
Without validation, a test can give results that look scientific but don’t guide care. That’s why the NHS doesn’t accept mycotoxin blood or urine testing — they haven’t been shown to make diagnoses more accurate or treatments more effective.
What if your mycotoxin test is positive, but you don’t live in a damp home?
This is very common.
-
Food is the main source: Mycotoxins are often found in grains, nuts, coffee, and dried fruit.
-
Exposure ≠ illness: A positive only shows contact, not harm.
-
No NHS role: Since the tests can’t separate harmless from harmful exposure, they aren’t used.
-
What matters most: If you’re unwell, validated NHS tests (CT scans, Aspergillus IgE/IgG, sputum cultures) guide proper diagnosis and treatment.
Foods that can contain mycotoxins
-
Aflatoxins – peanuts, maize, tree nuts, dried fruit, spices.
-
Ochratoxin A – coffee, dried fruit, wine, cereals.
-
Fumonisins, zearalenone, DON – maize, wheat, cereals.
-
Patulin – apples and apple juice.
-
Gliotoxin – made by Aspergillus fumigatus; occasionally found in mouldy cereals/silage, but mainly important when produced inside the body during invasive aspergillosis.
👉 In the UK/EU, foods are routinely monitored and regulated to keep levels very low.
What this means for patients
-
If you have aspergillosis or asthma, mould can worsen symptoms — but NHS doctors use validated tests, not private toxin panels.
-
If you feel unwell in a mouldy home, focus on fixing damp and talking to your GP or specialist.
-
A positive mycotoxin test without damp exposure almost always reflects normal diet.
-
Be cautious about spending money on unvalidated tests, which don’t change safe NHS treatment.
💙 Key message: Damp and mould can harm health, and sometimes mycotoxins are part of that story. But unvalidated mycotoxin blood/urine tests are unreliable and not used by the NHS. The safest approach is to fix damp, protect your lungs, and rely on NHS-approved diagnostics and treatments.
Glossary of Terms
-
WHO – World Health Organization, the UN’s global health authority.
-
CDC – Centers for Disease Control and Prevention, the main US public health body.
-
EMA – European Medicines Agency, which regulates medicines across the European Union.
-
MHRA – Medicines and Healthcare products Regulatory Agency, the UK body that regulates medicines and devices.
-
NHS – National Health Service, the publicly funded health system in the UK.
-
IgE / IgG – Immunoglobulin E and Immunoglobulin G, types of antibodies measured in blood tests to check for allergy or immune response.
-
CT scan – Computed Tomography scan, a detailed type of X-ray that shows cross-sections of the body.
-
MCAS – Mast Cell Activation Syndrome, a condition where mast cells release too many chemicals, causing allergic-type symptoms.
-
ABPA – Allergic Bronchopulmonary Aspergillosis, an allergic lung condition caused by reaction to Aspergillus.
-
CPA – Chronic Pulmonary Aspergillosis, a long-term fungal infection of the lungs caused by Aspergillus.