
When Caring for a Loved One Becomes Overwhelming: A Guide for Family Carers
Caring for a spouse, parent, or child is one of the most loving things you can do — but it can also be one of the hardest. Many family carers feel torn: wanting to give the very best care, yet struggling with exhaustion, isolation, and the feeling that “no one else can do it as well as me.”
This guide brings together insights to help you recognise when caring is becoming too heavy, why it feels so difficult to let go, and how to build a sustainable balance that protects both you and the person you love.
Why caring feels so demanding with family
-
Loss of independence: Illness often leaves people feeling powerless. Demanding behaviour can be a way of trying to regain control.
-
Role reversal stress: When a child becomes a parent’s carer, or a spouse becomes more like a nurse, both sides can feel uncomfortable.
-
Emotional safety: Patients often hold back with professionals but show raw feelings at home. That can come across as extra demanding.
-
Blurred boundaries: With family, it’s harder to say “no.” A patient may expect more than they ever would from an outsider.
When the caring role becomes unreasonable
Caring is no longer sustainable when:
-
Your health breaks down from exhaustion or stress.
-
You are completely isolated, with no time for friends, rest, or hobbies.
-
The caree’s demands exceed real need, and everything revolves around them.
-
Boundaries disappear and you can’t say no without conflict.
-
You are the only source of support, with no outside help.
These are warning signs that it’s time to rebalance the situation.
Why it doesn’t mean “defeat”
Asking for help can feel like admitting failure — but it isn’t.
-
Caring is a marathon, not a sprint. Protecting your health means you can keep caring longer.
-
Strength means knowing your limits. Bringing in help shows foresight, not weakness.
-
Love isn’t replaced. Professional carers can take tasks off your hands, but your relationship and bond remain uniquely yours.
Think of it not as “stepping back” but as building a care team. You remain the anchor, but you don’t carry everything alone.
Why it’s hard to let others help
Many carers say: “They don’t do it as well as I do.” This is natural — you know your loved one’s habits and needs better than anyone. Professionals may work differently, and that can feel uncomfortable.
But:
-
Different doesn’t always mean worse — just not “your way.”
-
Perfection isn’t sustainable if it destroys your health.
-
Your role as spouse/child/friend is irreplaceable — letting others handle routine care may free you to keep that role.
Start small: allow someone else to take over one task or cover for a short period. Gradually, trust can build.
Can problems be predicted?
Yes — carers often see the signs early:
-
Constant exhaustion or resentment
-
Dropping their own health needs or appointments
-
Losing touch with friends and community
-
Feeling guilty if they take any time for themselves
If these signs appear, it’s time to bring in extra support before crisis strikes.
Practical steps to make caring sustainable
-
Have early, honest conversations about what you can and cannot do.
-
Ask for a Carer’s Assessment (in the UK) — this can open up respite care, day services, and financial support.
-
Bring in professional support early so it feels like teamwork, not abandonment.
-
Protect your own time — even short, regular breaks keep you healthier.
-
Seek peer support — carers’ groups and counselling reduce isolation.
Final thought
Caring is an act of deep love. But love alone cannot carry the whole weight forever. Sharing the load is not defeat — it is the wisest way to ensure that both you and your loved one remain safe, cared for, and connected.
You are not failing. You are leading a team, protecting your own well-being, and preserving the relationship that matters most.
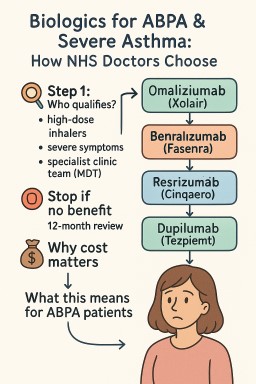
💊 Biologics for ABPA & Severe Asthma: How NHS Doctors Choose
Biologics are modern injection or infusion treatments that target the immune system. They can help people with Allergic Bronchopulmonary Aspergillosis (ABPA) by reducing inflammation, cutting down on steroid use, and lowering flare-ups.
In the UK, consultants must follow NICE (National Institute for Health and Care Excellence) guidance, which sets both clinical criteria and cost-effectiveness rules.
🔎 Step 1: Who qualifies?
-
You must already be on high-dose inhalers and still have severe symptoms.
-
Decisions are made by a specialist severe asthma / ABPA clinic team (MDT).
-
Blood tests, flare history, and steroid use are all considered.
🧭 Step 2: Which biologic?
Consultants match the drug to the type of inflammation you have:
| Pathway / Clues | Possible Biologic | Notes |
|---|---|---|
| IgE-allergic (allergic tests positive, high IgE) | Omalizumab (Xolair) | Works best if perennial allergies are driving symptoms. |
| Eosinophilic (high eosinophil counts, frequent flare-ups, or long-term steroid use) | Mepolizumab (Nucala) or Benralizumab (Fasenra) | NHS requires doctors to choose the least-expensive if both fit. |
| Eosinophils ≥400 + frequent flare-ups | Reslizumab (Cinqaero, IV drip) | Less used, but an option if IV therapy is acceptable. |
| Still severe after above / not eligible | Dupilumab (Dupixent) | Also helps if you have eczema or nasal polyps. |
| Any type, severe with ≥3 flare-ups or on daily steroids | Tezepelumab (Tezspire) | Works even if blood tests don’t show high eosinophils or IgE. |
🛑 Step 3: Stop if no benefit
NICE requires a 12-month review.
-
If your flare-ups or daily steroid dose haven’t fallen enough (usually by ≥50%), treatment should stop.
💷 Why cost matters
-
The NHS only funds biologics judged “cost-effective.”
-
If two drugs are equally suitable, consultants must use the least-expensive one.
-
This doesn’t mean you won’t get the right drug — but sometimes doctors must justify why one biologic is better for you personally.
📌 What this means for ABPA patients
-
ABPA is not directly covered by NICE guidance, but the same biologics are often used if you also meet asthma criteria.
-
Main goals:
-
Reduce oral steroids (prednisolone) and their side-effects.
-
Control flare-ups and lung damage.
-
-
Evidence supports omalizumab, mepolizumab, benralizumab, and dupilumab in ABPA; tezepelumab has less data so far.
✅ Bottom line:
Biologics can be life-changing for ABPA patients, but the NHS pathway means the choice depends on your blood results, flare history, steroid needs — and cost-efficiency rules. If one option doesn’t work, another may still be possible.
📚 New Children’s Book Helps Families Understand Aspergillosis
Launch Event at Affinity Outlet, Fleetwood – 13th September 2025
The Aspergillosis Trust is delighted to announce the launch of a brand-new children’s book, Dad and the Sneaky Spores, written by award-winning author Christina Gabbitas and beautifully illustrated by Ursula Hurst.
This story has been specially commissioned to raise awareness of aspergillosis, a serious lung condition caused by the Aspergillus fungus. Through gentle storytelling and colourful illustrations, the book helps children and families understand what it means to live with a parent affected by aspergillosis.
✨ About the Event
📅 Date: Saturday 13th September 2025
📍 Location: Affinity Outlet, Fleetwood
The launch event will be a fun and informative day for all the family.
-
✍️ Meet the Author: Christina Gabbitas will be signing copies of the book between 12pm and 2pm.
-
👩⚕️ Ask the Experts: A qualified nurse will be available to answer medical questions or offer advice.
-
📚 Learn Together: Families can explore how storytelling can make complex health conditions easier to understand.
📖 About Dad and the Sneaky Spores
The book follows a family’s journey with aspergillosis in a way that children can relate to. It not only explains the illness but also encourages empathy, resilience, and understanding within families.
“The narrative not only educates readers about aspergillosis but is also thoughtfully crafted to foster empathy and understanding.” – Aspergillosis Trust
Published by Poems & Pictures, Dad and the Sneaky Spores is available from 1st August 2025.
💜 Why This Matters
Aspergillosis is a rare and often misunderstood condition. By raising awareness through creative storytelling, this initiative provides a new way to start important conversations with children, families, and the wider community.
🔗 Find out more at: www.aspergillosistrust.org
Prednisone, Hydrocortisone, and Adrenal Function – What Patients Need to Know
Why Aspergillosis Patients Are Often Given Prednisolone
Prednisolone is often prescribed for patients with aspergillosis (especially Allergic Bronchopulmonary Aspergillosis – ABPA) because it helps to reduce lung inflammation and allergic reactions triggered by Aspergillus spores. It can be life-changing in controlling breathlessness, wheeze, and repeated flare-ups. However, using steroids for weeks or months can affect the body’s own natural hormone production.
How Do I Know If I Might Need Adrenal Testing While on Prednisolone?
Prednisolone is a corticosteroid medicine. If you take it for more than a few weeks, it can “switch off” your adrenal glands, which normally make the hormone cortisol. Cortisol is essential for coping with stress, fighting infection, and maintaining energy.
You might need adrenal testing if you notice:
-
Extreme tiredness or weakness, especially if it worsens when tapering your pred dose.
-
Excessive sleepiness or difficulty staying awake, even when rested.
-
Feeling much worse during stress or illness (for example, flu, chest infection, or surgery).
-
Dizziness or fainting on standing (low blood pressure symptoms).
-
Nausea, vomiting, or stomach pain that isn’t explained by infection or medicines.
-
Unexplained weight loss or poor appetite.
Why Might Patients Stop Making Cortisol?
The adrenal glands may temporarily stop producing cortisol if they have been “switched off” by long-term steroid treatment. This is called secondary adrenal insufficiency. It is usually reversible, but recovery can take months or even years.
In contrast, primary adrenal insufficiency (Addison’s disease) is when the adrenal glands are damaged and stop working permanently. This is not caused by steroids, but by autoimmune or other diseases.
Symptoms of Low DHEA
The adrenal glands also produce DHEA, a weak sex hormone that contributes to mood, energy, and libido — particularly important in women. Long-term steroid use or secondary adrenal insufficiency may reduce DHEA levels.
Possible signs of low DHEA:
-
Ongoing low energy or fatigue, even when cortisol is replaced
-
Low mood, depression, or “flat” emotions
-
Reduced libido (sex drive)
-
Thinning of underarm or pubic hair (especially in women)
-
Lower resilience or general sense of well-being
Not all patients with adrenal insufficiency need DHEA replacement, but in some, it can make a difference. This is assessed by specialists.
How to Tell the Difference Between Causes of Fatigue
Because fatigue can come from several overlapping sources, it helps to compare:
| Symptom | Cortisol deficiency (Adrenal Insufficiency) | Prednisolone Side Effect | Low DHEA |
|---|---|---|---|
| Sudden exhaustion during stress/illness | ✅ | ❌ | ❌ |
| Sleepiness, can’t stay awake | ✅ | ❌ | ❌ |
| Dizziness or fainting | ✅ | ❌ | ❌ |
| Nausea, vomiting, stomach upset | ✅ | ❌ | ❌ |
| Insomnia, wired-but-tired feeling | ❌ | ✅ | ❌ |
| Mood swings, irritability | ❌ | ✅ | ❌ |
| Weight gain, bloating, “puffy face” | ❌ | ✅ | ❌ |
| Ongoing low energy despite treatment | ❌ | ❌ | ✅ |
| Low mood, “flat” emotions | ❌ | ❌ | ✅ |
| Reduced libido | ❌ | ❌ | ✅ |
| Thinning pubic/underarm hair (women) | ❌ | ❌ | ✅ |
✅ = typical feature
Prednisolone, Hydrocortisone and Fatigue
-
If a patient is on prednisolone and feels extremely fatigued during stress or illness, it may mean their body is not making enough natural cortisol.
-
If they are tapering prednisolone and develop fatigue or sleepiness, this can mean the taper is too fast and the adrenal glands have not “woken up” yet.
-
If a patient feels tired while still on prednisolone, it could be due to:
-
Side effects of prednisolone itself,
-
Lack of natural cortisol (adrenal suppression),
-
Or low DHEA.
-
Treatment and Monitoring
-
Doctors may recommend slowing or pausing tapering if adrenal insufficiency is suspected.
-
Some patients are switched to hydrocortisone, which more closely mimics natural cortisol.
-
In situations of stress (infection, surgery, trauma), patients may need extra “stress doses” of steroids.
-
Patients at risk should carry a steroid emergency card or medical alert bracelet.
👉 Key message:
Aspergillosis patients often need steroids, but long-term use can suppress natural adrenal function. Fatigue can come from:
-
Low cortisol,
-
Prednisolone side effects,
-
Or low DHEA.
Since these overlap, specialist endocrine advice is often needed to work out the cause.

NHS England - You and Your GP: Key Points for NHS Patients Managing Aspergillosis
You and your general practice (YYGP) has been developed to help patients understand what to expect from their general practice and how they can get the best from their GP team. YYGP also enables patient to provide feedback or raise concerns with their GP Practice, Healthwatch or the integrated care board. The contract requires every GP practice to have linked to the NHS England YYGP document on their website, no later than 1 October 2025.
1. Accessing Your GP
-
Opening hours: Your GP is typically open 8:00 – 18:30, Monday to Friday. You can walk in, call, or use the NHS App or practice website to contact them NHS England.
-
If closed: For urgent but non-emergency needs, use 111 online or by calling 111 NHS England.
-
In an emergency: If symptoms are life-threatening (e.g., sudden severe breathing issues), go to A&E or call 999 NHS England.
2. Making an Appointment
-
When you contact your GP—whether by phone, online, or in person—they’ll assess your condition and respond within one working day with next steps NHS England.
-
This could include:
-
A face-to-face appointment
-
A phone consultation
-
A text message with advice
-
A recommendation to consult a pharmacy or another NHS service NHS England.
-
This prompt response is especially important for aspergillosis fluctuations or side effects from antifungal treatments.
3. Who You'll See
-
You may be seen by a GP, nurse, or pharmacist.
-
If you have a designated carer, they can speak on your behalf (with your permission).
-
If you prefer a specific healthcare professional you trust, request them—though waits might be longer NHS England.
-
Seeing the same clinician regularly can be beneficial for managing complex, long-term conditions like aspergillosis NHS England.
4. Support for Additional Needs
-
If English isn't your first language, you can request interpretation services when booking an appointment.
-
If you need extra help—like longer appointments, a quiet space, wheelchair access, or materials in accessible formats—just let the practice know; they'll try to accommodate NHS England.
5. Changing or Selecting a GP
-
You can find or switch to a GP using the NHS website (“Find a GP”) or by contacting local practices directly NHS England.
-
No ID, NHS number, or proof of address is needed to register—even if you’re homeless or your immigration status is uncertain NHS England.
-
If a practice cannot register you, they must explain their decision in writing within 14 days NHS England.
6. Referral and Treatment Flexibility
-
If your GP refers you to a specialist (e.g., respiratory consultant), you often have the right to choose your hospital or clinic NHS England.
7. Free Care & Private Work
-
GP services are free, including appointments and treatments.
-
Extra services like insurance letters may incur a fee NHS England.
8. Being a Helpful Patient
-
Prepare for appointments: list symptoms, treatment concerns, and questions in advance.
-
Be punctual or cancel in good time to avoid delays for others.
-
Use the NHS App or website to book appointments, refill prescriptions, and view test results.
-
Turn on App notifications to stay updated with messages from your practice NHS England.
-
Order repeat prescriptions well ahead—especially vital when managing antifungal medications—to avoid running out NHS England.
-
Consider joining the Patient Participation Group at your practice to share feedback and help improve services NHS England.
9. Sharing Feedback or Concerns
-
To raise concerns, talk to your practice manager first.
-
If needed, you can escalate feedback to your local Integrated Care Board (ICB).
-
You can also reach out to your local Healthwatch (an independent NHS watchdog) for confidential advice and support NHS England.
Why This Matters for Aspergillosis Patients
Aspergillosis often requires ongoing monitoring, regular breathing tests, imaging, and antifungal therapy adjustments. Timely access to GP services, continuity of care, and preparedness all enhance your ability to manage flare-ups or side effects effectively.
Handy Checklist (for easy reference)
| Task |
|---|
| Contact GP promptly for new or worsening symptoms |
| Prepare questions ahead—e.g., changes in breathing, treatment effects |
| Use NHS App to manage appointments and medications |
| Order repeat prescriptions early to maintain drug access |
| Request support services if needed (interpretation, accessibility) |
| Provide feedback to improve your experience and others' |
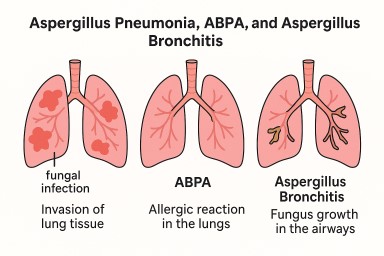
Other forms of aspergillosis: Aspergillus Pneumonia (Community-Acquired Aspergillus Lung Infection)
What is it?
Aspergillus pneumonia is a rare but serious lung infection caused by breathing in spores of the Aspergillus mould (most often Aspergillus fumigatus). Unlike allergic conditions such as Allergic Bronchopulmonary Aspergillosis (ABPA) or Aspergillus bronchitis, which affect the airways, Aspergillus pneumonia occurs when the fungus actually invades lung tissue. This makes it a more dangerous condition.
How do people catch it?
Most cases are acquired in the community (outside hospital).
You may be at higher risk if you have:
-
A weakened immune system (chemotherapy, transplant, high-dose steroids, uncontrolled diabetes).
-
Chronic lung disease such as COPD or emphysema.
-
A very heavy exposure to fungal spores (compost heaps, rotting bark, mulch, or farming dust).
Almost all cases are due to Aspergillus fumigatus, though other species like A. flavus have also been reported.
How common is it?
-
Aspergillus pneumonia is uncommon, despite Aspergillus spores being everywhere in the environment.
-
It is most often seen in people with weak immune defences, long-term lung disease, or very high exposure.
-
Because it often looks like ordinary bacterial or viral pneumonia, it can be missed or diagnosed late.
Symptoms
The illness may start like a regular chest infection:
-
Cough (dry or with sputum)
-
Shortness of breath
-
Fever or chills
-
Chest pain
-
Fatigue
-
Sometimes coughing up blood
It may progress:
-
Slowly over weeks, with cavities (holes) forming in the lungs.
-
Very quickly, especially after flu, COVID-19, or high spore exposure.
How does it differ from other Aspergillus conditions?
| Condition | What’s happening | Who gets it | Key signs |
|---|---|---|---|
| Aspergillus Pneumonia | Fungus invades lung tissue (serious infection) | Immunocompromised patients, COPD, heavy spore exposure | Pneumonia-like illness: fever, cough, breathlessness, chest pain |
| ABPA | Allergy to Aspergillus spores causes airway inflammation | People with asthma or cystic fibrosis | Wheeze, thick mucus plugs, recurrent asthma attacks |
| Aspergillus Bronchitis | Fungus grows in widened/damaged airways without invading tissue | People with bronchiectasis or chronic airway disease | Chronic cough, mucus, sometimes blood streaks |
👉 In short:
-
Pneumonia = infection inside lung tissue (dangerous, urgent).
-
ABPA = allergic reaction in the lungs.
-
Bronchitis = long-term airway infection.
Is it a type of invasive aspergillosis?
Yes. Aspergillus pneumonia is considered a form of invasive aspergillosis because the fungus invades lung tissue:
-
Acute/severe form: fast, aggressive illness in very vulnerable people (immunocompromised, post-viral, heavy spore exposure).
-
Subacute or “necrotising” form: slower, smouldering infection in people with COPD, diabetes, or long-term steroids, often with cavities.
👉 It is not mild like ABPA or bronchitis — it requires antifungal treatment.
Diagnosis
Doctors may use:
-
Chest X-ray or CT scan – patches, cavities, or diffuse shadowing.
-
Sputum or bronchoscopy samples – to detect Aspergillus in culture or under the microscope.
-
Blood tests – for Aspergillus antibodies, or sometimes antigen (galactomannan).
Treatment
-
Antifungal medicines are the main treatment (voriconazole is most common; sometimes itraconazole or posaconazole).
-
Corticosteroids may be added in severe “pneumonitis-type” illness with overwhelming inflammation.
If treatment begins early, many people respond well. If diagnosis is delayed, the illness can progress rapidly and be life-threatening.
Outlook
-
Without antifungal treatment, Aspergillus pneumonia can be fatal.
-
With modern antifungal drugs, survival and recovery are possible.
-
Some people may develop long-term lung damage, even after successful treatment.
Key message for patients
If you have sudden worsening cough, fever, or chest symptoms that don’t improve with antibiotics — especially if you have COPD, are on steroids, or have had heavy spore exposure — ask your doctor whether Aspergillus pneumonia should be considered. Early diagnosis and treatment make the best outcomes possible.
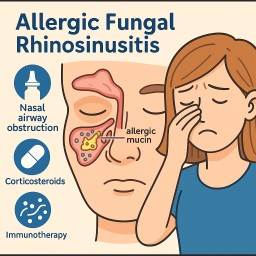
Other types of aspergillosis: Allergic Fungal Rhinosinusitis (AFRS)
(Also called Allergic Fungal Sinusitis, Allergic Aspergillus Sinusitis, Allergic Aspergillosis of the sinuses)
What is AFRS?
AFRS is a type of chronic sinus disease caused by an allergic reaction to fungi such as Aspergillus. It mainly affects adolescents and young adults, especially in warm and humid climates. AFRS accounts for about 5–10% of all cases of chronic sinusitis.
Unlike some other forms of fungal sinus disease, AFRS occurs in people with a normal immune system. It is not the same as an invasive fungal infection.
Symptoms
Common symptoms include:
-
Blocked or congested nose
-
Nasal polyps (soft swellings inside the nose)
-
Post-nasal drip (mucus running down the back of the throat)
-
Loss of smell or taste
-
Recurrent sinus infections
-
Headache or facial pressure
Pain is not typical — if severe pain is present, bacterial sinusitis may also be involved. Some people may have more dramatic problems such as worsening eye symptoms, changes in facial appearance, or very severe nasal blockage.
Diagnosis
Doctors may use a combination of:
-
CT scans showing thickened sinuses with “allergic mucin” (thick mucus mixed with fungal debris).
-
Nasal endoscopy to look for polyps and mucus.
-
Laboratory tests for raised IgE (allergy antibody) or specific IgE against fungi.
-
Biopsy or mucus samples, which sometimes show fungal filaments (though not always).
The diagnosis is sometimes difficult, as not every laboratory can reliably detect fungi in mucus.
Causes
AFRS is caused by an overactive immune response to fungi in the sinuses.
-
The most common fungi are Aspergillus (especially A. flavus), Alternaria, and Curvularia.
-
People with allergies, asthma, or nasal polyps are at higher risk.
Treatment
Treatment usually combines surgery and medical therapy.
-
Surgery: Performed using an endoscope through the nose. The aims are to:
-
Remove thick mucus and fungal debris.
-
Improve drainage and ventilation of the sinuses.
-
Allow future cleaning and access if disease comes back.
-
-
Steroids: Corticosteroids are used to control inflammation and prevent relapse. These may be:
-
Tablets (short or long courses depending on severity)
-
Nasal steroid sprays or rinses (usually long-term)
-
-
Other treatments:
-
Antifungal medicines are not clearly proven to help but may be tried in some cases.
-
Immunotherapy (allergy desensitisation) may help reduce recurrence.
-
Antibiotics such as azithromycin are occasionally added if bacteria are thought to play a role.
-
Despite treatment, recurrence is common. Many patients need repeat surgery or ongoing medical therapy.
Link with ABPA (Allergic Bronchopulmonary Aspergillosis)
AFRS affects the sinuses, while ABPA affects the lungs, but both are caused by an allergic reaction to Aspergillus and have many similarities.
-
Some patients develop both AFRS and ABPA, sometimes called “sinobronchial allergic mycosis syndrome.”
-
If you have AFRS and also develop asthma, persistent cough, or changes on a lung scan, your doctor may check for ABPA.
-
Likewise, people with ABPA and severe sinus symptoms may be assessed for AFRS.
-
If there is concern, your doctors may refer you to the National Aspergillosis Centre (NAC) in Manchester for specialist advice.
Key points for patients
-
AFRS is not a dangerous invasive infection, but it is long-lasting and tends to come back.
-
Surgery plus steroid treatment is the main approach.
-
Ongoing follow-up is important because relapse is common.
-
AFRS and ABPA can sometimes occur together, so chest symptoms should always be discussed with your doctor.
Other forms of aspergillosis: Chronic Aspergillus Sinusitis
(Chronic invasive and granulomatous forms)
Chronic sinus problems are very common, but in a small number of people they are caused by fungal infection, especially Aspergillus. This type of infection is different from the usual bacterial sinusitis and needs different treatment.
What is chronic Aspergillus sinusitis?
-
Chronic rhinosinusitis (CRS) is long-term inflammation of the sinuses (lasting more than 12 weeks).
-
In about 6–12% of CRS cases, fungi are the cause — with Aspergillus being the most common.
-
There are two important invasive forms that are rare but serious:
-
Chronic invasive Aspergillus sinusitis – the fungus grows slowly into the lining of the sinuses and nearby tissues.
-
Chronic granulomatous Aspergillus sinusitis – the immune system forms a hard granuloma (lump of immune cells and fungus), usually caused by Aspergillus flavus.
-
These conditions progress slowly but can cause long-term damage if not treated.
Who gets it?
-
Chronic invasive Aspergillus sinusitis is more common in Western countries and Japan.
-
Granulomatous sinusitis is more often seen in parts of Africa, South Asia (India, Pakistan), the Middle East, and occasionally the southern United States.
-
People at risk include:
-
Those with diabetes, on long-term steroids, or with HIV infection.
-
Sometimes people with no obvious immune problems can still develop it.
-
-
Aspergillus fumigatus usually causes chronic invasive sinusitis.
-
Aspergillus flavus is the main cause of granulomatous sinusitis.
Symptoms
Because these forms progress slowly, symptoms are often missed or mistaken for “ordinary sinus problems.” They may include:
-
Blocked or congested nose that doesn’t improve with usual treatments
-
Facial pain or pressure, especially around the eyes, cheeks, or forehead
-
Headaches
-
Nasal discharge, sometimes blood-stained
-
Bleeding from the nose (epistaxis)
-
Facial swelling or numbness
-
Bulging eye (proptosis) or reduced vision if the infection spreads to the orbit
-
Rarely: brain involvement (abscess, meningitis, stroke-like symptoms)
Granulomatous sinusitis often causes a slowly enlarging mass in the nose, cheek, or orbit, and may be mistaken for a tumour.
How is it diagnosed?
-
Scans (CT or MRI): show a mass in the sinuses, sometimes with bone damage. MRI is useful if the eye or brain are involved.
-
Endoscopy and biopsy: tissue samples are taken from the sinus lining.
-
Laboratory tests:
-
Special stains and fungal culture help identify Aspergillus.
-
Blood tests (Aspergillus IgG antibodies) can support the diagnosis.
-
-
Diagnosis can be delayed because the condition is uncommon and mimics other sinus problems.
Treatment
Prompt treatment is essential to prevent serious complications. Management usually involves:
-
Surgery
-
To remove infected tissue and improve sinus drainage.
-
Surgery also allows biopsy to confirm diagnosis.
-
-
Antifungal medication
-
Long-term antifungal tablets (usually itraconazole or voriconazole).
-
Sometimes intravenous antifungals (e.g. amphotericin B or posaconazole) are used in severe cases.
-
Treatment usually lasts at least 6 months, often longer (sometimes up to a year).
-
-
Managing risk factors
-
Good control of diabetes.
-
Reducing or stopping steroid medicines if possible.
-
Outlook (prognosis)
-
With early diagnosis and combined treatment (surgery + antifungals), many patients do well.
-
Granulomatous sinusitis tends to relapse more often but generally has a better long-term outlook than invasive sinusitis.
-
Regular follow-up is essential because recurrence is common.
-
Follow-up usually includes scans every few months and nasal endoscopy to check for regrowth.
-
Ongoing monitoring may be needed for up to 5 years.
-
Key points for patients
-
Chronic Aspergillus sinusitis is rare, but important to recognise because it needs different treatment than ordinary sinus infections.
-
Symptoms can mimic chronic sinusitis or even cancer, so biopsy and specialist review are essential.
-
Surgery plus antifungal medication is the main treatment.
-
Long-term follow-up is needed to monitor for relapse.
-
If you have risk factors like diabetes or steroid use, controlling these is important.
✅ Summary:
Chronic invasive and granulomatous Aspergillus sinusitis are rare but serious fungal infections of the sinuses. They progress slowly, can cause damage to the eyes or brain if untreated, and are sometimes mistaken for tumours. With specialist care, surgery, antifungal therapy, and long-term follow-up, most patients can achieve good control of the disease.
Other forms of aspergillosis: Aspergilloma (Fungal Ball in the Lung)
Aspergilloma (Fungal Ball in the Lung)
An aspergilloma is a clump of fungus (usually Aspergillus) that grows inside an old cavity in the lung. These cavities often form after conditions like tuberculosis (TB), other lung infections, or lung disease. The fungus does not usually invade healthy lung tissue, but it uses the cavity as a space to grow.
How common is aspergilloma?
-
Aspergillomas are uncommon overall, but they are more likely to appear in people who have had tuberculosis in the past.
-
In some countries where TB is (or was) common, aspergillomas are found quite frequently.
-
In countries like the UK, they are rare, but can still happen in people with conditions such as COPD, sarcoidosis, or after lung surgery.
-
Doctors often describe aspergilloma as part of the wider group of conditions called chronic pulmonary aspergillosis (CPA).
What are the symptoms?
-
Many people with an aspergilloma have very few symptoms at first – sometimes only a cough.
-
The most serious problem is bleeding from the lungs (haemoptysis). This can range from small streaks of blood in the sputum to heavy, life-threatening bleeding.
-
Some people may also have chest infections, breathlessness, or tiredness if other lung problems are present.
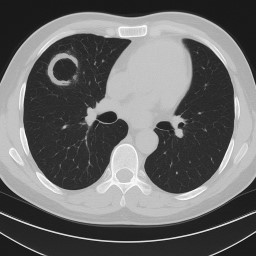
How is it found?
-
An aspergilloma usually shows up on a chest scan (X-ray or CT).
-
It often looks like a round “ball” inside a cavity in the upper part of the lung.
-
Sometimes it can move around a little inside the space.
-
Important note: Aspergillomas are not cancer, but they can sometimes be mistaken for cancer on scans. For this reason, doctors may arrange extra tests (such as blood tests, repeat scans, or sometimes biopsy) and may refer patients to the National Aspergillosis Centre (NAC) to be certain of the diagnosis.
Who looks after you?
-
At your local hospital, aspergillomas are usually managed by a respiratory (chest) specialist doctor.
-
Depending on your situation, they may also work with:
-
Thoracic surgeons (for possible surgery)
-
Radiologists (for scans or embolisation)
-
Infectious diseases doctors (for antifungal treatment)
-
-
If your case is complex, unclear, or high-risk, your local team can refer you to the National Aspergillosis Centre (NAC) at Wythenshawe Hospital, Manchester. NAC is the UK’s only NHS specialist centre for aspergillosis and provides expert diagnosis, advanced testing, and treatment advice, often working alongside your local hospital team.
What is the outlook (prognosis)?
-
Some aspergillomas remain stable for years and cause very few problems.
-
A small number may even disappear on their own, although this is unusual.
-
The main risk is serious bleeding, which can be sudden. This is why regular check-ups are important.
-
Surgery to remove the part of lung with the aspergilloma is usually the most effective treatment and can be curative in suitable patients.
-
For people who cannot have surgery, treatments such as blocking bleeding vessels (embolisation) or instilling antifungal medicine into the cavity can sometimes help, but problems may return.
🚨 Emergency: If you cough up blood 🚨
-
Small streaks of blood (mild):
-
Stay calm – these often stop by themselves.
-
Contact your hospital team promptly to let them know.
-
Keep a record of how much and how often it happens.
-
-
More than a few teaspoons, clots, or ongoing bleeding (moderate to heavy):
-
Call 999 (UK) or go to A&E immediately.
-
Sit upright to help protect the other lung.
-
Take this leaflet or your aspergillosis care details with you.
-
-
Very heavy bleeding (life-threatening):
-
Treat this as an emergency.
-
Emergency doctors may use medicine to help blood clot, a procedure to block the bleeding vessel (embolisation), or surgery if possible.
-
⚠️ Always report any bleeding to your doctor, even if it seems small.
Treatment options
-
No treatment may be needed if the aspergilloma is small, not causing bleeding, and the person feels well. Regular monitoring is important.
-
Surgery is the most effective treatment if the fungal ball is causing repeated or heavy bleeding.
-
Antifungal tablets are sometimes used before or after surgery, but on their own they are usually not very effective.
-
Tranexamic acid – a medicine that helps the blood clot – is sometimes prescribed to reduce or control bleeding. It can be taken by mouth or given in hospital if bleeding is significant. It does not remove the aspergilloma but can help keep bleeding under control.
-
Other treatments for people who cannot have surgery include:
-
Blocking the bleeding blood vessels (embolisation) – this can stop bleeding, but the effect may not last.
-
Instilling antifungal medicine directly into the cavity – less common, results vary.
-
Key points for patients
-
An aspergilloma is not cancer, but because it can sometimes look like cancer on scans, careful checks and sometimes referral to the NAC are needed.
-
The main risk is bleeding, which may require urgent treatment.
-
Surgery offers the best chance of cure, but only if lung function allows.
-
If you have an aspergilloma, you should:
-
Attend regular hospital check-ups.
-
Report any coughing up of blood immediately.
-
Take tranexamic acid if prescribed for bleeding, but also inform your doctor if bleeds occur.
-
Avoid blood-thinning medicines (like aspirin, ibuprofen, or some herbal remedies) unless your doctor prescribes them.
-

Shared Care Records in the NHS: What Aspergillosis Patients Need to Know
The NHS is changing how patient records are managed. By 2026, every area of England will have a Shared Care Record. This is not one big “national record,” but a way of securely linking together the different records held by your GP, hospital, and other services.
For patients with aspergillosis, this could make a real difference to care, safety, and research.
🗂 What Is a Shared Care Record?
-
Not one single file: Your GP, hospital, and community services keep their own systems.
-
Linked together: Clinicians can securely view a joined-up picture of your health.
-
Safer and faster care: Your allergies, test results, and medications can be seen wherever you are treated.
-
You tell your story once: No more repeating details every time you see a new doctor.
🛡 How Safe Is My Data?
-
Strict access control: Only staff directly involved in your care can open your record.
-
Audit trail: Every time it’s viewed, the system records who, when, and why.
-
Encryption & firewalls: Records are locked against outside access.
-
No mass downloads: Systems only allow one patient’s record at a time.
In many ways, this is safer than old paper notes, which could be lost, copied, or seen by accident.
👩⚕️ Confidentiality Rules Stay the Same
-
NHS staff are bound by confidentiality laws and the Caldicott Principles.
-
Looking at a record without a valid care reason is a disciplinary offence.
-
Your record is not shared with insurers, employers, or relatives without your consent.
📊 Research and Aspergillosis
Shared Care Records could also help improve research into aspergillosis, which is often under-recognised:
-
Better case finding: Linking GP, hospital, and lab data makes it easier to identify true cases.
-
Tracking outcomes: Researchers can follow IgE/IgG results, CT changes, and treatment responses over time.
-
Environmental links: Data could be combined with housing, air quality, and weather information.
-
Support for trials: Easier to find eligible patients for new antifungal or biologic studies.
All research use is usually de-identified (your name and personal details removed). You can choose to opt out via the National Data Opt-Out if you don’t want your data used in this way.
🏦 Will Insurance Companies See My Record?
No. Insurance companies and employers cannot access your NHS record.
If you apply for insurance, your GP may be asked for a report — but this is only done with your consent.
🌐 What If I Don’t Use the Internet?
You don’t need to be online to benefit. Shared Care Records are mainly for clinicians, not for patients logging in.
If you want to see your record, you can still ask for a paper copy from your GP or hospital.
📍 Who Runs Shared Care Records?
They are organised locally by Integrated Care Systems (ICSs).
-
England is divided into 42 ICSs, each bringing together NHS services, local councils, and community care.
-
Examples include Greater Manchester ICS, Cheshire & Merseyside ICS, and North East London ICS.
-
Scotland, Wales, and Northern Ireland use different systems.
✅ Key Reassurances for Patients with Aspergillosis
-
Your data remains confidential and secure.
-
Shared Care Records mean joined-up, safer care across GP, hospital, and community services.
-
Insurers and employers cannot access your NHS record.
-
You stay in control — you can opt out of data use for research if you wish.
-
The new system could help advance aspergillosis research, leading to better diagnosis and treatments.