📘 What is CPA? (Chronic Pulmonary Aspergillosis)
Patient handout for A&E staff who are not aware of aspergillosis.
What is CPA?
CPA is a chronic fungal infection of the lungs caused by Aspergillus, most often in people who already have damaged lungs from conditions like tuberculosis, COPD, lung cancer, or sarcoidosis.
Unlike ABPA, CPA is a true infection, not an allergic reaction. It is not contagious but can slowly destroy lung tissue if not treated.
Symptoms
-
Chronic cough, often with mucus
-
Coughing up blood (haemoptysis)
-
Fatigue, low-grade fever
-
Unexplained weight loss
-
Breathlessness
-
Recurrent chest infections not responding to antibiotics
Diagnosis
-
CT scan of the chest showing cavities, nodules, or fungus balls (aspergillomas)
-
Aspergillus IgG antibody (usually raised)
-
Positive sputum PCR or culture for Aspergillus
-
Exclude TB and malignancy
Treatment
-
Long-term antifungal therapy (e.g. itraconazole, voriconazole, posaconazole)
-
Monitor blood levels and liver function
-
Surgery or embolisation if severe bleeding occurs
-
Supportive care: oxygen, nutrition, physiotherapy
Key Points for A&E:
✅ CPA is a progressive fungal infection, not a typical bacterial pneumonia
✅ May present with haemoptysis, respiratory distress, or systemic illness
✅ Review current antifungal treatment and potential drug interactions
✅ Consider urgent chest CT and specialist referral if patient is unwell
📍 For specialist support:
National Aspergillosis Centre (NAC)
🏥 Wythenshawe Hospital, Manchester University NHS Foundation Trust
🌐 NAC homepage on MFT website https://mft.nhs.uk/wythenshawe/services/infectious-diseases/national-aspergillosis-centre/
🌐 www.aspergillosis.org
📞 Daytime contact: 0161 291 2891 or 0161 291 4362
📞 Urgent out-of-hours: Call Wythenshawe switchboard on 0161 998 7070
📢 Ask for the on-call Infectious Diseases Consultant
📘 What is ABPA? (Allergic Bronchopulmonary Aspergillosis)
Patient handout for A&E staff who ask what aspergillosis is.
What is ABPA?
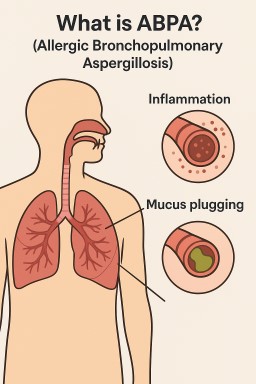
ABPA is an allergic lung condition caused by the immune system overreacting to the fungus Aspergillus. It mainly affects people with asthma or cystic fibrosis.
When Aspergillus spores are inhaled, most people clear them without issue. In ABPA, the immune system sees these spores as dangerous and mounts a strong inflammatory response. This leads to asthma-like symptoms, mucus plugging, and can result in permanent lung damage (bronchiectasis) if left untreated.
Symptoms
-
Worsening breathlessness
-
Wheezing, chest tightness
-
Coughing up thick, often brown mucus
-
Fever, fatigue, or feeling generally unwell
-
Unintentional weight loss (advanced cases)
Diagnosis
-
History of asthma or cystic fibrosis
-
High IgE levels and positive Aspergillus-specific IgE
-
Eosinophilia (raised white blood cells)
-
Sputum culture or PCR positive for Aspergillus
-
Chest imaging showing mucus plugging or bronchiectasis
Treatment
-
Oral corticosteroids (e.g. prednisolone) to reduce inflammation
-
Antifungal medication (e.g. itraconazole) to lower fungal burden
-
Biologic therapies (e.g. omalizumab or benralizumab) in some patients
-
Regular monitoring by respiratory or infectious diseases specialists
Key Points for A&E:
✅ ABPA is an allergic lung disease, not a classical infection
✅ Can present with severe asthma, mucus plugging, or type 2 respiratory failure
✅ Requires early recognition and often systemic steroids and antifungal therapy
✅ Take bloods (IgE, eosinophils, CRP), consider chest imaging, and review oxygen status
📍 For specialist support:
National Aspergillosis Centre (NAC)
🏥 Wythenshawe Hospital, Manchester University NHS Foundation Trust
🌐 NAC homepage on MFT website https://mft.nhs.uk/wythenshawe/services/infectious-diseases/national-aspergillosis-centre/
🌐 www.aspergillosis.org
📞 Daytime contact: 0161 291 2891 or 0161 291 4362
📞 Urgent out-of-hours: Call Wythenshawe switchboard on 0161 998 7070
📢 Ask for the on-call Infectious Diseases Consultant

Debate: Gender Bias in Science and Clinical Trials & Why It Matters to Patients
Introduction: A History of Exclusion For decades, medical research and clinical trials were built around a default male body. Women were routinely excluded from studies out of concern for hormonal variation, pregnancy risks, or assumptions that female responses would mirror male ones. The consequences? Misdiagnoses, incorrect dosing, side effects overlooked in women, and entire conditions dismissed as psychological.
This pattern of systemic gender bias has had real-life consequences for millions of women, especially those living with chronic or misunderstood illnesses like ME/CFS (Myalgic Encephalomyelitis/Chronic Fatigue Syndrome), long COVID, autoimmune diseases — and potentially, aspergillosis.
Section 1: Real Consequences of Exclusion
Why Gender Bias Matters in Asthma and Aspergillosis
Both asthma and aspergillosis are diseases where gender can influence immune response, disease progression, and side effects of treatment. Women are more likely to develop certain asthma subtypes (e.g., late-onset eosinophilic asthma), which overlap with allergic fungal conditions like ABPA. They may also experience more frequent exacerbations and are more vulnerable to long-term steroid side effects such as adrenal insufficiency and bone loss. Despite this, sex-specific analysis is rare in fungal disease trials, and asthma research has only recently begun to explore these differences.
Is Gender Relevant in Aspergillosis? While aspergillosis affects people of all sexes, some patterns suggest potential sex differences in prevalence, diagnosis, immune response, and treatment side effects:
- Chronic Pulmonary Aspergillosis (CPA) appears more common in men, especially in post-TB or COPD populations, but women may experience more severe fatigue or be underdiagnosed.
- In ABPA (Allergic Bronchopulmonary Aspergillosis), hormonal differences may influence disease severity, and women often report more exacerbations or sensitivity to long-term steroid treatment.
- Invasive aspergillosis is less well studied for sex differences, though some research in animal models suggests hormonal influences on fungal immunity.
- Women may also be more vulnerable to side effects of antifungals and corticosteroids, such as adrenal suppression, hearing loss, or osteoporosis.
Despite these observations, most clinical studies do not stratify by sex or explore gender-specific differences, leaving important questions unanswered.
A Message to Women Living with Aspergillosis
If you're reading this as a woman affected by aspergillosis, please don’t feel discouraged. While we highlight gaps in past research, the goal is to push for better inclusion, not to suggest you're being overlooked in care. You are not alone. Clinicians are becoming more aware of these issues, and researchers — especially in the UK — are actively working to close the gender gap. Patient groups and specialist centres like the NAC are also strong advocates for fair, personalised treatment. Your voice matters, and being informed is a powerful step in making future care better for everyone.
Clinical trials that exclude or underrepresent women have led to:
- Drugs that stay longer in women's bodies (e.g., Zolpidem) causing next-day drowsiness and driving risk
- Heart medications being under-prescribed to women, because early trials only studied men
- Misunderstanding of how autoimmune diseases develop and respond to treatment
- Failure to understand symptoms unique to women, such as how heart attacks present differently
Historically, women were also more likely to have their physical symptoms dismissed as anxiety or "hysteria." ME/CFS, a condition affecting mostly women, was dismissed for decades as psychological. When patients with ME later caught COVID-19, many were again left behind as new post-viral syndromes took priority.
For patients with aspergillosis, particularly chronic forms like CPA or ABPA, the relevance is clear. These conditions are under-researched and under-recognised, and early studies may not fully reflect how they impact women. Steroid-related side effects like osteoporosis, adrenal suppression, and hearing loss may differ by sex — yet sex-stratified data is rarely available.
Section 2: Has Anything Changed?
Yes. In the UK, the National Institute for Health and Care Research (NIHR) and the Medical Research Council (MRC) have taken steps to improve inclusion:
- NIHR-funded studies are expected to include representative populations and report on diversity
- UK Research and Innovation (UKRI) promotes equality in trial design, including sex and gender analysis
- The DecodeME study (the world’s largest ME/CFS genetics study, based in the UK) is actively engaging with female participants
But gaps remain — especially in rare diseases, chronic illnesses, and reproductive health. For fungal disease and aspergillosis specifically, many trials still do not analyse sex-specific outcomes, despite women forming a significant proportion of the affected population.
Section 3: Are Women Now Being Protected Too Much? Some worry that extra precautions — like excluding women from early-phase trials — may backfire:
- Delaying access to life-changing drugs
- Forcing women to wait until post-marketing surveillance to be included
- Excluding pregnant and breastfeeding women entirely, even when they are at high risk (e.g., in pandemics)
This creates a paradox: either women are harmed by being ignored, or excluded "for their safety."
The solution is not to avoid studying women — but to design smarter, safer, inclusive trials from the beginning.
Section 4: Will We Need Two Trials — One for Men, One for Women? This concern is understandable. Stratifying data by sex, running subgroup analyses, and including both pre- and post-menopausal women does cost more.
But it's not about running two separate trials. It's about:
- Recruiting balanced numbers of men and women
- Analysing sex-specific outcomes from one trial
- Designing adaptive trials or pooled data studies
Neglecting sex differences costs more in the long run — through failed drugs, recalls, and harm to patients.
Section 5: Positive Examples of Progress
- UK heart disease research now includes female-specific risk factors and symptom profiles in NICE guidance
- Autoimmune research increasingly uses female animal models and stratifies analysis by sex
- Endometriosis, menopause, and menstrual health are finally getting targeted research funding in the UK
- DecodeME is helping uncover the genetic basis of ME/CFS with full inclusion of women
- Long COVID clinics in the NHS are building on lessons from women-led ME/CFS research
- New studies on asthma and fungal allergy (e.g., ABPA) are beginning to explore hormonal and immunological factors that may differ by sex
Section 6: Where Patients Fit In Patients have led many of these changes:
- Women with ME, long COVID, POTS, or fibromyalgia have insisted their experiences are real
- Advocacy groups in the UK (e.g. Action for M.E., LongCovidSOS, National Aspergillosis Centre support groups) have pushed for sex-specific research
- Patient-led data collection and patient involvement in trial design are now expected in NIHR-funded studies
- In rare fungal diseases like CPA, SAFS, and ABPA, patients can support research by contributing to trials that welcome women and report on sex-specific outcomes
Conclusion: A Call to Patients This isn’t just a scientific issue — it’s a patient rights issue. Without full inclusion of women in research, we can't expect safe, effective, and equitable treatments.
Ask questions. Share your stories. Advocate for better science. And when possible, participate in trials that commit to transparency and inclusivity.
For patients with aspergillosis, the message is clear: We need sex-aware, inclusive research to understand this complex disease in all its forms — and that means including and reporting on women properly.
Medicine must work for everyone — not just the default male.
💭 Why Some People with Aspergillosis Delay Going to A&E
And Why That Could Be Dangerous
If you live with chronic aspergillosis — whether CPA, ABPA, SAFS, or aspergillus bronchitis — you’ve probably had moments where your symptoms suddenly worsened and you didn’t know what to do. Maybe you’ve thought about going to A&E, or even dialling 999, but something stopped you.
You're not alone. Many people in our community feel reluctant to seek emergency care, even when they’re very unwell.
Here’s why — and why it matters.
🏥 “I’ve Been to A&E Before — and It Wasn’t a Good Experience”
Many patients have told us:
-
“I waited for hours just to be told it’s probably my usual symptoms.”
-
“The staff didn’t seem to know what aspergillosis is.”
-
“They didn’t know how to manage my antifungal treatment or asthma.”
-
“I felt dismissed — like I was being dramatic.”
Experiences like this can leave people feeling humiliated or unsafe, and understandably less likely to go back — even when things are serious.
🛏️ “I Don’t Want to Be Admitted — I’ll Be Stuck There”
A&E can be a gateway to hospital admission, and for someone managing a complex, fluctuating condition at home, this can feel like losing control. You may worry about:
-
Being put on the wrong ward
-
Catching infections
-
Not being given the right antifungal, steroid, or oxygen support
-
Losing time, independence, or confidence
So instead, you might choose to stay home — sometimes too long.
⌛ “I Don’t Want to Waste Anyone’s Time”
We hear this all the time:
“A&E is for people who are really ill — not for someone like me.”
“The NHS is already overwhelmed.”
“I’ll just give it a bit more time.”
But remember: you’re not wasting time by going to A&E if your health is deteriorating. Chronic illness doesn’t make your emergency less urgent — it just makes it harder to spot.
😔 “I’m Tired of Needing Help”
Living with chronic aspergillosis is exhausting. It’s easy to feel like:
-
“I should be able to manage this myself.”
-
“I don’t want to be a burden.”
-
“It’s probably just another bad flare.”
But when symptoms cross a line — from “bad day” to “dangerous” — it’s vital to act. Seeking urgent care isn’t failure. It’s strength.
🌫️ “I Didn’t Know It Was That Serious”
The truth is: even very experienced patients often aren’t sure when symptoms need emergency treatment. You might think:
-
“I’ve had breathlessness before — I’ll just rest.”
-
“The coughing is worse, but it’s happened before.”
-
“I’ll wait until the morning and see.”
But if you’re coughing blood, can’t speak a sentence, can’t stand up, or feel confused or faint, waiting is dangerous.
💬 “I Asked in a Group First”
Support groups are amazing — and a lifeline for many. But no group can diagnose an emergency. If you're:
-
Asking whether to go to A&E
-
Describing symptoms that sound like respiratory failure, sepsis, or adrenal crisis
-
Hoping someone tells you not to worry...
Then it’s already time to act, not wait for replies.
✅ Final Message
If you have severe symptoms, sudden changes, or feel frightened about your health:
Don’t wait. Don’t post. Don’t hope it passes.
Call 999 or go to A&E.
You are not a burden. You are not overreacting.
You are saving your own life.
When to go to A&E or call 999

🚨 When to Go to A&E or Call 999
A Guide for People with Chronic Aspergillosis, Asthma, and Other Long-Term Conditions
When you live with a long-term health condition like chronic aspergillosis (CPA), allergic bronchopulmonary aspergillosis (ABPA), severe asthma, or immunosuppression, it can be hard to know when a flare-up is “just part of the illness” — and when it’s something more serious that needs emergency medical care.
This guide is designed to help you — or someone you care for — recognise the signs that mean it’s time to stop waiting, stop asking for online advice, and get help immediately.
🧠 A Special Note for People with Aspergillosis
People living with chronic aspergillosis often get used to symptoms like breathlessness, coughing, fatigue, or chest tightness. That makes it easy to miss or downplay serious changes — especially if you're reluctant to make another trip to A&E.
But there are times when acting fast is critical.
If you have CPA, ABPA, SAFS, or aspergillus bronchitis, you should go to A&E or call 999 immediately if you experience:
-
🫁 Sudden or worsening breathlessness, especially if it’s different from your usual
-
💨 Breathing that doesn’t improve after using inhalers, nebulisers, or oxygen
-
💔 New chest pain or tightness — particularly if it spreads or worsens when breathing
-
🌡️ A high fever, shaking chills, or flu-like symptoms
-
🩸 Coughing up blood — especially if it's fresh or in large amounts
-
🧠 Feeling confused, drowsy, or faint
-
❗ Severe weakness, fatigue, or inability to stand or walk
-
💊 Severe reaction to medications (e.g. antifungals, steroids, or biologics) — rash, swelling, dizziness, jaundice
⚠️ Don’t Wait or Ask Online — Act Fast When These Signs Appear
We completely understand why some people — particularly those with severe asthma, CPA, or ABPA — may be hesitant to go to A&E. You may have faced:
-
Long waits
-
Feeling dismissed or misunderstood
-
Fear of hospital admission
-
Exhaustion from too many medical appointments
These are real concerns, but when you're struggling to breathe, disoriented, or deteriorating rapidly, it’s not the time to post in a support group or wait for reassurance. It’s time to act.
In life-threatening moments, what you need isn’t advice — it’s treatment.
No support group — no matter how compassionate — can replace oxygen, IV antibiotics, a steroid boost, or emergency care.
Please don’t delay. You are never wasting anyone’s time by seeking help when something feels wrong.
🔥 Emergency Symptoms That Always Need 999 or A&E
Whether you have a long-term condition or not, there are symptoms that require immediate action:
🫁 Breathing Problems
-
Severe breathlessness, even at rest
-
Struggling to speak or complete sentences
-
Gasping, wheezing, choking
-
Blue or grey lips, face, or fingertips
-
No response to inhalers or nebulisers
-
Sudden onset shortness of breath
❤️ Chest Pain or Heart Symptoms
-
Crushing or heavy chest pain
-
Pain radiating to jaw, neck, arms, or back
-
Palpitations + fainting, dizziness, or breathlessness
-
Fast or irregular heartbeat
-
Suspected heart attack or angina
🧠 Neurological Emergencies
-
Sudden weakness or numbness (especially on one side)
-
Slurred speech, facial droop, or confusion
-
Seizures or fits (especially if new or lasting >5 minutes)
-
Sudden, severe headache
-
Loss of consciousness or collapse
🌡️ Infection / Sepsis Signs
-
High fever with chills or rigors
-
Very fast breathing or heartbeat
-
Cold, mottled, clammy skin
-
Feeling very drowsy, confused, or unable to stay awake
-
Not passing urine or drinking
-
Feeling like something is seriously wrong
🩸 Bleeding or Trauma
-
Heavy bleeding that doesn’t stop
-
Major burns or deep wounds
-
Suspected broken bones
-
Head, neck, or spinal injury
-
Bleeding from eyes, genitals, or rectum
💊 Medication-Related Emergencies
-
Anaphylaxis: swelling, rash, shortness of breath, collapse
-
Adrenal crisis (especially in those on long-term steroids): vomiting, confusion, weakness, fainting
-
Severe side effects to antifungals or biologics: dizziness, liver pain, rash, yellowing skin
-
Sudden change in behaviour or mental state after a new medication
🧭 Not Sure? Here's What to Do
-
If you’re in doubt, but worried: Call NHS 111
-
If symptoms are severe, worsening, or causing distress: Call 999 or go to A&E
-
If you’re alone, unwell, and unsure — you are safer being checked
📘 Summary: When to Get Help Immediately
| Symptom Area | Emergency Signs |
|---|---|
| Aspergillosis-specific | Sudden breathlessness, new chest pain, coughing blood, fever, severe weakness, confusion |
| Breathing | Gasping, cyanosis, wheezing unrelieved by inhalers |
| Heart | Chest pain, palpitations with collapse, irregular pulse |
| Neurological | Stroke signs, seizures, new confusion, severe headache |
| Infection/Sepsis | High fever + confusion or fast breathing, cold mottled skin |
| Trauma/Bleeding | Uncontrolled bleeding, deep wounds, broken bones, burns |
| Medication-related | Anaphylaxis, adrenal crisis, severe side effects, sudden mental health change |
💬 Final Word
If you're experiencing any of these symptoms, this is not the time to post in a support group or wait to see how things go.
Please don’t delay — even if you’ve had difficult A&E experiences in the past. The risk of waiting is far greater than the discomfort of being seen.
You are never wasting anyone’s time by protecting your health or saving your life.
💬 What Would Help You Consider Taking Part in a Clinical Trial?
As part of the aspergillosis community — whether you're a patient, carer, or supporter — your voice matters. We’d like to ask:
What would make you feel more confident or willing to consider taking part in a clinical trial?
We’re not asking you to sign up.
We’re asking you to help us understand what matters — so we can make trials feel safer, clearer, and more patient-friendly for everyone.
🧠 We Understand the Hesitations
Over the years, we’ve heard a range of understandable concerns:
-
“Will I be safe?”
-
“Will this interfere with my current treatment?”
-
“What if it’s a waste of time?”
-
“I don’t want to be pressured or used.”
Some of this worry comes from the way trials have been presented in the past, or from media coverage about vaccines or experimental drugs. And we get it — it’s not easy to agree to something unknown, especially when your health is already fragile.
🧭 But Trials Can’t Happen Without You — and in Aspergillosis, It’s Especially Difficult
The reality is:
It’s harder than ever to find people willing to take part in clinical trials.
And for a condition like aspergillosis, that challenge is even greater.
Why?
-
It’s a rare condition, so there are fewer eligible patients
-
It’s a complex condition, often involving other lung diseases, steroid use, or immunosuppression
-
People living with aspergillosis often deal with unpredictable flare-ups, fatigue, or long-term medication side effects, which can make the idea of extra appointments or uncertainty even harder
Even when promising new treatments (like biologics or inhaled antifungals) are ready to be tested, many trials can’t go ahead — or finish — because not enough people can or are willing to volunteer.
This means slower progress, longer waits for new treatment options, and missed opportunities for care to improve.
🙏 So We’re Asking You:
If you’ve ever taken part in a trial — what helped you say yes?
If you haven’t — what would you need in order to even consider it?
Would it help to:
-
Know more about your rights and safety?
-
Speak to someone who’s done it before?
-
Read a simple explanation of what the trial involves?
-
Have the option to talk it through without pressure?
Whatever your answer — it matters.
💡 Would a "Patients for Clinical Trials" Page on Aspergillosis.org Help?
We’re thinking of creating a page that would:
-
Explain what clinical trials are (and aren’t) — in plain English
-
Share real stories from patients who’ve taken part
-
Offer clear information about trial opportunities — without pressure
-
Answer your most common questions honestly
-
Give you a place to register interest or ask questions — even anonymously
Would something like that make a difference for you?
What would it need to include to feel useful, safe, and respectful?
💬 Help Us Get This Right
We’re not asking you to sign up.
We’re asking for your input.
Because the biggest thing holding back better treatment for aspergillosis is not the science — it’s how hard it is to find people willing or able to take part.
That’s no one’s fault. But we’d like your help to improve it.
You can reply in the support group, message us privately, or fill out an anonymous form (coming soon).
🧩 Together, We Can Make Trials More Patient-Centred
Your feedback could:
-
Help new patients feel less afraid
-
Improve how trials are explained
-
Make the process more flexible, respectful, and supportive
Because better treatments for aspergillosis start with listening — and they start with you.
Click here to add your comments or suggestions
🦠 Understanding Antibiotic Use in Aspergillosis: A Guide to Antimicrobial Stewardship (AMS)
This information is provided to help you understand your treatment. Always follow your medical team's advice. They will make the best decision for your care based on your individual health needs.
⚖️ What is Antimicrobial Stewardship (AMS)?
Antimicrobial stewardship means using antibiotics responsibly — only when needed, and choosing the most appropriate one for each infection. This helps protect patients from side effects and helps ensure antibiotics remain effective in the future.
For people with chronic lung conditions like chronic pulmonary aspergillosis (CPA), ABPA, or aspergillus bronchitis, this balance is especially important.
🔍 Why Is This Important for Aspergillosis Patients?
-
Antibiotics don’t work for fungal infections, but they may be prescribed if a bacterial infection is also present.
-
Using unnecessary antibiotics can lead to side effects, gut upset, or drug interactions (especially with antifungal medicines).
-
Overuse of broad-spectrum antibiotics can make future infections harder to treat.
Your clinical team carefully considers all of this when prescribing.
🔴 Broad-Spectrum Antibiotics
Broad-spectrum antibiotics target a wide range of bacteria, including helpful ones in your body. They are sometimes necessary, but their use is carefully monitored.
| Examples | Common Uses |
|---|---|
| Co-amoxiclav | Chest infections, dental issues |
| Ciprofloxacin, Levofloxacin | Serious or hospital infections |
| Doxycycline | Chest infections, acne |
| Azithromycin | Atypical pneumonia |
| Meropenem | Resistant or hospital-acquired infections |
🧠 These antibiotics may be used only if clearly needed. Doctors will often review and adjust the treatment after tests.
🟢 Narrow-Spectrum Antibiotics
These target specific bacteria and are usually first choice when the infection source is known.
| Examples | Common Uses |
|---|---|
| Penicillin V | Sore throats, dental infections |
| Flucloxacillin | Skin infections (e.g. infected eczema) |
| Nitrofurantoin | Urinary tract infections |
| Vancomycin (IV) | Resistant bacterial infections |
| Fosfomycin | Resistant urinary infections |
✅ These are often preferred because they reduce the risk of resistance and protect your body’s healthy bacteria.
🤝 What You Can Do
-
Trust your clinical team’s decisions — they are based on guidelines, test results, and your health history.
-
Tell your doctor or pharmacist about all medications you are taking — especially antifungals like itraconazole or voriconazole.
-
Report any side effects or concerns, especially if you notice gut problems or unexpected symptoms.
⚠️ A Note on Drug Interactions
Some antibiotics (like clarithromycin or rifampicin) can reduce how well azole antifungals work. Your doctor will avoid these combinations or adjust treatment accordingly.
✅ Final Reminder
This article is for general understanding only.
Your doctors are trained to choose the safest and most effective treatments for your condition. If you’re ever unsure about why a medication has been prescribed, ask — they’ll be happy to explain.
💡 Dupilumab for ABPA: What You Need to Know Now the Trial Is Complete
A large Phase III trial—called LIBERTY‑ABPA AIRED—has recently completed studying dupilumab in people with ABPA and asthma who frequently exacerbate despite other treatments. Let’s break down what that means and what’s still missing 📌
🗓️ Trial Timeline & Scope
-
Trial completed: Primary data collection finished in July 2023, study closed in February 2024. It enrolled around 170 patients from over 30 sites across several countries including the UK, EU, US, Canada, Japan, and more Wikipedia+15trialsummaries.com+15Clinical Trials Register+15.
-
Design: Randomized, double‑blind, placebo‑controlled over 52 weeks, followed by 12 weeks safety follow‑up trialsummaries.comClinical Trials Register.
📋 What Was Measured?
The trial assessed:
-
Severe respiratory exacerbations (requiring steroids or hospital admission)
-
Lung function changes (e.g. FEV₁)
-
ABPA-related symptoms, quality of life, asthma control
-
Biomarkers including IgE and FeNO
-
Safety and tolerability, including antibody formation to dupilumab Wikipedia+15Clinical Trials+15trialsummaries.com+15
🧬 Why Results Matter
Dupilumab blocks both IL‑4 and IL‑13 pathways, which drive inflammation, mucus, and elevated IgE in ABPA. Early case reports and small series have shown promising benefits, especially in reducing exacerbations and steroid use, but until now, no large randomized trial data were available ScienceDirect+1PMC+1.
❓ What’s Available Now?
-
✅ The trial has finished, but official results have not yet been published or released publicly.
-
🕒 Regulators and sponsors previously estimated publication around late 2023, with actual report likely still under review or preparation ctv.veeva.com+3ScienceDirect+3Clinical Trials+3.
-
📡 Until these results are public, dupilumab remains not officially approved for ABPA, though individual clinicians may consider off‑label use in select cases.
🧾 Summary Table: Where Things Stand
| Status | Current Position |
|---|---|
| Trial status | Completed Feb 2024 |
| Official results | Pending publication |
| Based on early data | Case reports show improvement in exacerbations and steroid reduction |
| Regulatory status | Not yet licensed for ABPA treatment |
| Clinical use now | Only as part of research or off‑label under specialist review |
💬 What Should Patients Do Now?
If you’re managing ABPA and considering biologic options:
-
✅ Ask if longstanding biologics like dupilumab are being considered for your individual case.
-
💬 Be clear that formal approval for ABPA is still pending, pending public release of the trial results.
-
🩺 Consult with your specialist or asthma/respiratory team about possible off‑label use—they can explain access options, benefits, and risks.
🧭 Final Thoughts
The LIBERTY‑ABPA AIRED trial has now completed, marking a major milestone for potential new treatment in ABPA. But until results are published and reviewed, dupilumab remains off-label for this condition.
You may still hear about its use in ABPA from case reports showing positive outcomes—but wider clinical acceptance awaits published study data. If it becomes available, it could offer meaningful benefits—but only if confirmed in research.

🤐 Why It's Important Not to Share Your Clinical Trial Experience — Until It’s Over
If you have chronic pulmonary aspergillosis (CPA), you may be invited to take part in a clinical trial for a new antifungal medication like rezafungin. That’s exciting — and could help improve treatment for many people in future.
Naturally, people want to support each other by sharing experiences, especially in online support groups. But when it comes to clinical trials, there’s a really important reason why we shouldn’t talk about how we’re feeling while we’re still in the trial.
Here’s why.
🧪 What Are Clinical Trials For?
Clinical trials help doctors and researchers answer important questions like:
-
Does this new treatment work?
-
Is it better than the current treatment?
-
What side effects might it cause?
To get accurate answers, the trial needs to be fair and unbiased — meaning that personal expectations and outside influences shouldn’t affect how people report their symptoms or progress.
📣 The Problem With Sharing During a Trial
If you’re taking part in a trial and say something like:
“I feel great — this new drug is working for me!”
or
“This is making me feel worse than ever — don’t join!”
...other people may change how they think and feel based on your comment.
This is called bias. It can:
-
Make others expect the same good (or bad) result
-
Affect how people rate their own symptoms
-
Cause people to drop out or not join at all
-
Make the trial results less accurate or even unusable
Even well-meaning comments can damage the study, especially if the trial is small (like most CPA studies are).
🕵️♀️ What If It’s a Blinded Trial?
Some trials are "blinded", meaning you don’t know whether you're getting the new treatment or a standard one (or placebo).
But if people start guessing or posting:
“I’m sure I’m on the real drug — I feel amazing!”
...then other people might also guess, or feel disappointed — which again, affects how results are reported.
🚦When Is It Safe to Share?
💬 After the trial is over and the results are published, you can talk freely about your experience.
In fact, patient voices are vital at that stage — they help others understand what it’s like to be part of a trial and whether new treatments are helpful in real life.
💡 What You Can Say During the Trial
You can still help raise awareness without compromising the study. For example:
-
✅ “I’m taking part in a CPA trial – ask your doctor if you might be eligible.”
-
✅ “There’s a study on a new antifungal — here’s the link to the official trial page: clinicaltrials.gov/study/NCT06794554”
-
✅ “I’m proud to be contributing to research — happy to share my experience once the trial ends.”
Just don’t talk about how the treatment is affecting you until the trial is complete.
🙏 Why This Matters
By keeping quiet during the trial, you're:
-
Protecting the integrity of the study
-
Helping future patients get trustworthy answers
-
Supporting the research team who need clear, unbiased data
You’re not just taking part in a trial — you’re helping build evidence that others will depend on for years to come.
🧭 Summary
| ✅ Do | ❌ Don’t |
|---|---|
| Tell people a trial exists | Share how the treatment is affecting you |
| Encourage others to talk to their doctor | Post guesses about which drug you’re on |
| Wait until the trial ends to share experiences | Influence others to join based on your results |
If you're ever unsure, ask your clinical trial team or group moderator — they'll be glad to help. Your role in research is important, and your silence now is a powerful act of support for science, fairness, and future care.

🧾 Rezafungin: A New Antifungal Being Trialled for CPA
Some people with chronic pulmonary aspergillosis (CPA) have trouble tolerating standard antifungal medications. Commonly used drugs like voriconazole and posaconazole can cause serious side effects such as hallucinations, liver enzyme disturbances, or gut problems. When these medications can’t be used, options become limited.
A new antifungal, rezafungin, is now being studied as a possible treatment for CPA — especially in people who can't tolerate azoles. It is not yet approved for aspergillosis, but a major clinical trial is under way.
🧬 What Is Rezafungin?
Rezafungin is part of a newer group of antifungal drugs called echinocandins. These work by weakening the fungal cell wall — a very different mechanism to azole drugs like itraconazole or voriconazole.
Key features:
-
Given as a weekly intravenous (IV) drip
-
Long-acting: stays in the body for days after each dose
-
Designed to provide high drug levels in the lungs and bloodstream
-
Early studies show less frequent side effects than with some older antifungals
It is already licensed for treatment of Candida bloodstream infections but is being studied now for CPA.
🧪 Current Research: Trial for CPA
A clinical trial is currently recruiting people with CPA who:
-
Cannot take azole antifungals because of side effects or resistance
-
Need alternative or combination therapy
This trial (called REZAFUNGin Efficacy and Safety for Aspergillus – CPA) is being conducted in the UK and internationally. The goal is to test whether rezafungin is safe and effective in CPA patients who have few remaining options.
🔗 View the clinical trial (NCT06794554)
📊 What Have Previous Studies Found?
While studies in CPA are just beginning, previous trials in other fungal infections provide important clues:
✅ Phase 2 & 3 Studies (Candida Infections)
-
Rezafungin was found to be as effective as daily echinocandins (like caspofungin)
-
Once-weekly dosing worked just as well as daily treatment
-
Side effects were mild, and liver toxicity was rare
-
No CNS side effects (like hallucinations) were reported
🧫 Laboratory Evidence
-
Rezafungin is active against Aspergillus fumigatus, including some azole-resistant strains
-
It reaches good levels in lung tissue — an important feature for CPA
-
May be used alone or with another antifungal in complex cases
🩺 Case Example
A recent case report described successful treatment of chronic pulmonary aspergillosis using rezafungin plus voriconazole in a patient with resistant infection (Oxford University Press, 2024).
⚠️ Is Rezafungin Available Now?
Not yet. Rezafungin is only available for CPA:
-
Through a clinical trial, or
-
By special approval for compassionate use in selected cases
It is not currently licensed for aspergillosis in the UK or elsewhere.
💬 What Should I Discuss with My Doctor?
If you're considering participation in a clinical trial or if standard treatments have failed, you might ask:
-
Am I eligible for the rezafungin CPA trial?
-
What are the benefits and risks of trying this treatment?
-
Will I still need other antifungals (e.g. azoles or amphotericin)?
-
How often will I need blood tests and hospital visits?
-
Will this help if I have azole resistance or liver side effects?
📌 Summary
Rezafungin is a new antifungal drug being tested for people with chronic pulmonary aspergillosis who cannot take older treatments. It offers once-weekly dosing and early signs suggest a favourable safety profile, including in patients with liver concerns or those who had side effects from azoles.
Although not yet widely available, it may offer hope for people with limited options. If you or someone you know is struggling with antifungal intolerance, you may wish to speak to your medical team about the CPA clinical trial or explore compassionate access routes.
👉 Learn more or check trial sites:
🔗 https://clinicaltrials.gov/study/NCT06794554