Other forms of aspergillosis: Aspergilloma (Fungal Ball in the Lung)
Aspergilloma (Fungal Ball in the Lung)
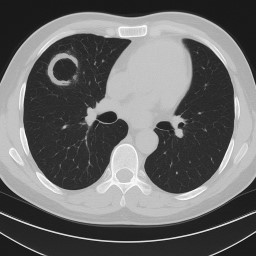
An aspergilloma is a clump of fungus (usually Aspergillus) that grows inside an old cavity in the lung. These cavities often form after conditions like tuberculosis (TB), other lung infections, or lung disease. The fungus does not usually invade healthy lung tissue, but it uses the cavity as a space to grow.
How common is aspergilloma?
-
Aspergillomas are uncommon overall, but they are more likely to appear in people who have had tuberculosis in the past.
-
In some countries where TB is (or was) common, aspergillomas are found quite frequently.
-
In countries like the UK, they are rare, but can still happen in people with conditions such as COPD, sarcoidosis, or after lung surgery.
-
Doctors often describe aspergilloma as part of the wider group of conditions called chronic pulmonary aspergillosis (CPA).
What are the symptoms?
-
Many people with an aspergilloma have very few symptoms at first – sometimes only a cough.
-
The most serious problem is bleeding from the lungs (haemoptysis). This can range from small streaks of blood in the sputum to heavy, life-threatening bleeding.
-
Some people may also have chest infections, breathlessness, or tiredness if other lung problems are present.
How is it found?
-
An aspergilloma usually shows up on a chest scan (X-ray or CT).
-
It often looks like a round “ball” inside a cavity in the upper part of the lung.
-
Sometimes it can move around a little inside the space.
-
Important note: Aspergillomas are not cancer, but they can sometimes be mistaken for cancer on scans. For this reason, doctors may arrange extra tests (such as blood tests, repeat scans, or sometimes biopsy) and may refer patients to the National Aspergillosis Centre (NAC) to be certain of the diagnosis.
Who looks after you?
-
At your local hospital, aspergillomas are usually managed by a respiratory (chest) specialist doctor.
-
Depending on your situation, they may also work with:
-
Thoracic surgeons (for possible surgery)
-
Radiologists (for scans or embolisation)
-
Infectious diseases doctors (for antifungal treatment)
-
-
If your case is complex, unclear, or high-risk, your local team can refer you to the National Aspergillosis Centre (NAC) at Wythenshawe Hospital, Manchester. NAC is the UK’s only NHS specialist centre for aspergillosis and provides expert diagnosis, advanced testing, and treatment advice, often working alongside your local hospital team.
What is the outlook (prognosis)?
-
Some aspergillomas remain stable for years and cause very few problems.
-
A small number may even disappear on their own, although this is unusual.
-
The main risk is serious bleeding, which can be sudden. This is why regular check-ups are important.
-
Surgery to remove the part of lung with the aspergilloma is usually the most effective treatment and can be curative in suitable patients.
-
For people who cannot have surgery, treatments such as blocking bleeding vessels (embolisation) or instilling antifungal medicine into the cavity can sometimes help, but problems may return.
🚨 Emergency: If you cough up blood 🚨
-
Small streaks of blood (mild):
-
Stay calm – these often stop by themselves.
-
Contact your hospital team promptly to let them know.
-
Keep a record of how much and how often it happens.
-
-
More than a few teaspoons, clots, or ongoing bleeding (moderate to heavy):
-
Call 999 (UK) or go to A&E immediately.
-
Sit upright to help protect the other lung.
-
Take this leaflet or your aspergillosis care details with you.
-
-
Very heavy bleeding (life-threatening):
-
Treat this as an emergency.
-
Emergency doctors may use medicine to help blood clot, a procedure to block the bleeding vessel (embolisation), or surgery if possible.
-
⚠️ Always report any bleeding to your doctor, even if it seems small.
Treatment options
-
No treatment may be needed if the aspergilloma is small, not causing bleeding, and the person feels well. Regular monitoring is important.
-
Surgery is the most effective treatment if the fungal ball is causing repeated or heavy bleeding.
-
Antifungal tablets are sometimes used before or after surgery, but on their own they are usually not very effective.
-
Tranexamic acid – a medicine that helps the blood clot – is sometimes prescribed to reduce or control bleeding. It can be taken by mouth or given in hospital if bleeding is significant. It does not remove the aspergilloma but can help keep bleeding under control.
-
Other treatments for people who cannot have surgery include:
-
Blocking the bleeding blood vessels (embolisation) – this can stop bleeding, but the effect may not last.
-
Instilling antifungal medicine directly into the cavity – less common, results vary.
-
Key points for patients
-
An aspergilloma is not cancer, but because it can sometimes look like cancer on scans, careful checks and sometimes referral to the NAC are needed.
-
The main risk is bleeding, which may require urgent treatment.
-
Surgery offers the best chance of cure, but only if lung function allows.
-
If you have an aspergilloma, you should:
-
Attend regular hospital check-ups.
-
Report any coughing up of blood immediately.
-
Take tranexamic acid if prescribed for bleeding, but also inform your doctor if bleeds occur.
-
Avoid blood-thinning medicines (like aspirin, ibuprofen, or some herbal remedies) unless your doctor prescribes them.
-

Shared Care Records in the NHS: What Aspergillosis Patients Need to Know
The NHS is changing how patient records are managed. By 2026, every area of England will have a Shared Care Record. This is not one big “national record,” but a way of securely linking together the different records held by your GP, hospital, and other services.
For patients with aspergillosis, this could make a real difference to care, safety, and research.
🗂 What Is a Shared Care Record?
-
Not one single file: Your GP, hospital, and community services keep their own systems.
-
Linked together: Clinicians can securely view a joined-up picture of your health.
-
Safer and faster care: Your allergies, test results, and medications can be seen wherever you are treated.
-
You tell your story once: No more repeating details every time you see a new doctor.
🛡 How Safe Is My Data?
-
Strict access control: Only staff directly involved in your care can open your record.
-
Audit trail: Every time it’s viewed, the system records who, when, and why.
-
Encryption & firewalls: Records are locked against outside access.
-
No mass downloads: Systems only allow one patient’s record at a time.
In many ways, this is safer than old paper notes, which could be lost, copied, or seen by accident.
👩⚕️ Confidentiality Rules Stay the Same
-
NHS staff are bound by confidentiality laws and the Caldicott Principles.
-
Looking at a record without a valid care reason is a disciplinary offence.
-
Your record is not shared with insurers, employers, or relatives without your consent.
📊 Research and Aspergillosis
Shared Care Records could also help improve research into aspergillosis, which is often under-recognised:
-
Better case finding: Linking GP, hospital, and lab data makes it easier to identify true cases.
-
Tracking outcomes: Researchers can follow IgE/IgG results, CT changes, and treatment responses over time.
-
Environmental links: Data could be combined with housing, air quality, and weather information.
-
Support for trials: Easier to find eligible patients for new antifungal or biologic studies.
All research use is usually de-identified (your name and personal details removed). You can choose to opt out via the National Data Opt-Out if you don’t want your data used in this way.
🏦 Will Insurance Companies See My Record?
No. Insurance companies and employers cannot access your NHS record.
If you apply for insurance, your GP may be asked for a report — but this is only done with your consent.
🌐 What If I Don’t Use the Internet?
You don’t need to be online to benefit. Shared Care Records are mainly for clinicians, not for patients logging in.
If you want to see your record, you can still ask for a paper copy from your GP or hospital.
📍 Who Runs Shared Care Records?
They are organised locally by Integrated Care Systems (ICSs).
-
England is divided into 42 ICSs, each bringing together NHS services, local councils, and community care.
-
Examples include Greater Manchester ICS, Cheshire & Merseyside ICS, and North East London ICS.
-
Scotland, Wales, and Northern Ireland use different systems.
✅ Key Reassurances for Patients with Aspergillosis
-
Your data remains confidential and secure.
-
Shared Care Records mean joined-up, safer care across GP, hospital, and community services.
-
Insurers and employers cannot access your NHS record.
-
You stay in control — you can opt out of data use for research if you wish.
-
The new system could help advance aspergillosis research, leading to better diagnosis and treatments.
🩺 NHS Data Sharing: How It Will Improve Your Care
🌍 The Problem Today
At the moment, your health information is stored in many different places:
-
Your GP (General Practitioner) has one record.
-
Hospitals keep their own records.
-
Community services (like district nurses or physiotherapists) have separate notes.
-
Social care also keeps its own information.
This can cause problems:
-
You may be asked to repeat your story again and again.
-
Doctors don’t always see the full picture (medications, allergies, past test results).
-
Sometimes tests are repeated unnecessarily.
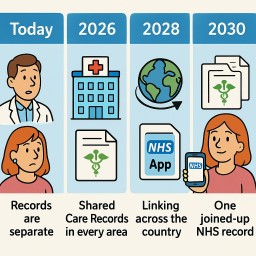
📅 The Timeline for Change
Today (2025)
-
Records are mostly separate.
-
Some areas already share basic information like your medicines and allergies through a “Summary Care Record.”
👉 What it means for you: You still have to repeat information at most appointments.
2026 – Shared Care Records in Every Area
-
Every region (called an Integrated Care System, or ICS) will have a Shared Care Record.
-
This links together information from GPs, hospitals, community teams, and social care.
-
Hospitals using modern systems like Epic (a type of electronic patient record - MFT has installed this already) can also start sharing directly with other Epic hospitals.
👉 What it means for you: Doctors can see more of your health record without asking you to repeat everything.
2028 – Linking Across the Country
-
Regional Shared Care Records will start to connect with each other.
-
Epic hospitals across the UK will share records more easily using Care Everywhere (Epic’s sharing tool).
-
Community services and “virtual wards” (hospital care at home) will be fully connected.
👉 What it means for you: If you are treated in another part of the country, staff there will be able to see important parts of your health record straight away.
2030 – One Joined-Up NHS Record
-
The NHS plans to give every patient a longitudinal record – one joined-up health and care record that follows you everywhere.
-
This will combine information from GPs, hospitals, community services, mental health teams, and social care.
-
Patients will also be able to see much more of their own record through the NHS App.
👉 What it means for you: Wherever you go in the NHS, staff can see your medical history safely. You’ll feel your care is joined-up, and you can also check your record yourself.
✅ Your Patient Journey: Step by Step
-
Today: “I have to explain my medication list every time. I’m not sure my hospital knows what my GP prescribed.”
-
2026: “When I go into hospital, the doctor can already see my GP record and community nurse notes.”
-
2028: “I was treated far from home, and the hospital could see my recent test results straight away.”
-
2030: “Wherever I go, the NHS staff have the full picture. I can see my record too on the NHS App.”

Why It Can Be Hard to Clear Carbon Dioxide (CO₂) From the Lungs in Aspergillosis
When we breathe, oxygen comes in and carbon dioxide (CO₂) goes out. For people living with aspergillosis (ABPA or CPA), and sometimes with other conditions like severe asthma, COPD, or bronchiectasis, this process can be much more difficult.
🔴 Why this happens
-
Narrow or inflamed airways
In ABPA or asthma, swelling and tightening of the breathing tubes can trap air inside. -
Collapsed or floppy airways
In COPD and bronchiectasis, airways may close too soon when you breathe out, leaving CO₂ stuck in the lungs. -
Mucus and plugs
Thick or sticky mucus — common in ABPA, bronchiectasis, and COPD — blocks airways and reduces airflow. -
Scarred or damaged lungs
CPA can create cavities and scarring that make air movement less efficient. -
Tired breathing muscles and fatigue
Long-term illness, steroid use, or simple exhaustion can weaken the diaphragm and chest muscles, making it harder to breathe out fully.
🟢 What can help
-
Pursed-lip breathing
Inhale gently through your nose, then breathe out slowly through pursed lips (like blowing out a candle). This keeps airways open longer so CO₂ can escape. -
Diaphragm (belly) breathing
Using your stomach muscles for slower, deeper breaths improves oxygen and CO₂ exchange. -
Clear the mucus
Daily airway clearance (physio techniques, huff coughing, or devices like Acapella, Flutter, Aerobika) can stop mucus building up and blocking airways. -
Pulmonary rehabilitation
Specialist exercise and breathing training improve stamina, breathing control, and lung efficiency. -
Find the best position
Sitting upright or leaning forward slightly often makes it easier to breathe out during flare-ups. -
Medical treatments
Your team may use antifungals, steroids, inhalers, or nebulisers to reduce inflammation and mucus.
If CO₂ levels remain too high, oxygen therapy or breathing support machines (like BiPAP or CPAP) may be needed.
👩⚕️ Who can help most
The best place for personalised advice is usually a respiratory physiotherapist.
They can:
-
Teach you the right breathing techniques
-
Show you how to clear your airways effectively
-
Support you with safe exercise and pacing strategies
🟦 What to do if you panic for breath
Feeling panic when breathless is common — but panic can make breathing even harder. Try these steps:
-
Stop and sit upright — lean slightly forward with your arms supported on a table or your knees.
-
Focus on breathing out — use pursed-lip breathing (in through the nose, out slowly through pursed lips).
-
Slow things down — count “in for 2, out for 4” to calm breathing.
-
Loosen tight clothing — open collars or waistbands to ease pressure on the chest.
-
Use your reliever inhaler or nebuliser if prescribed.
-
Stay calm with grounding techniques — focus on your surroundings (e.g. name things you see or hear) to reduce panic.
⚠️ When to seek urgent help
-
If your breathing does not improve after following these steps.
-
If you are too breathless to speak in full sentences.
-
If you feel faint, confused, or unusually drowsy.
-
If you have sudden chest pain or start coughing up a lot of blood.
➡️ Call 999 or go to A&E immediately in these situations.
✅ Key message
For patients with aspergillosis, especially when combined with asthma, COPD, or bronchiectasis, clearing CO₂ can be harder because of blocked or damaged airways, mucus, and fatigue.
-
Learning breathing techniques
-
Clearing mucus regularly
-
Seeking advice from a respiratory physiotherapist
-
Knowing what to do if you panic for breath
…can all make a big difference in helping you breathe more easily and safely.
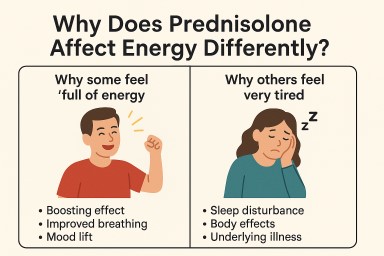
Why Does Prednisolone Affect Energy Differently?
If you live with aspergillosis, you may be prescribed prednisolone, a type of steroid medicine that reduces inflammation in the lungs. Many patients notice changes in their energy levels — but not everyone experiences the same effects.
Why some feel “full of energy”
-
Boosting effect: Prednisolone can act a bit like adrenaline, raising blood sugar and speeding up metabolism.
-
Improved breathing: When inflammation in the lungs is brought under control, it may feel easier to breathe, which can make you more energetic.
-
Mood lift: In some people, steroids can trigger feelings of alertness or even mild euphoria.
Why others feel very tired
-
Sleep disturbance: Prednisolone can interfere with your normal sleep pattern, especially if taken later in the day. Poor sleep = daytime fatigue.
-
Body effects: Steroids can cause muscle breakdown, fluid changes, or blood sugar swings, which may leave you feeling drained.
-
Adrenal suppression: If you’ve been on steroids for a while, your body’s own cortisol production may slow down, leading to tiredness, especially during dose reductions.
-
Underlying illness: Even if the steroid helps, aspergillosis itself (with coughing, infections, or bleeding) can still leave you exhausted.
What you can do
-
Take in the morning: This reduces the chance of sleep problems.
-
Plan rest breaks: Listen to your body if you’re feeling tired.
-
Track your symptoms: Notice if your energy changes when doses go up or down.
-
Talk to your doctor: If you feel extremely fatigued or “too wired to sleep,” your team may be able to adjust your dose, timing, or taper.
✅ Key message for patients:
It is normal for people with aspergillosis to respond differently to prednisolone — some feel more energetic, while others feel exhausted. Both reactions are common. If the effects are troubling, discuss them with your medical team so your treatment can be adjusted safely.
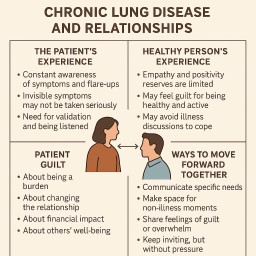
Chronic Lung Disease and Relationships: The Emotional Impact for Patients, Partners, Friends & Family
Living with chronic lung disease — such as ABPA, CPA, bronchiectasis, or severe asthma — affects far more than the body.
It alters the emotional landscape between the person with the illness and the people around them.
This isn’t just about physical limitations — it’s about how empathy, energy, guilt, and emotional resilience are shared (or strained) over time.
This guide explores both perspectives — the patient and the healthy person — and offers ways to keep relationships strong.
1. The Patient’s Perspective
For the person with the illness, the condition is ever-present:
-
Constant awareness – Every breath, plan, or activity is influenced by symptoms, medication schedules, and the risk of flare-ups.
-
Invisible symptoms – You can feel like you’re drowning without looking or sounding breathless. The absence of obvious signs often means people underestimate how unwell you are.
-
Need for validation – Being listened to, believed, and taken seriously is essential. Dismissive comments such as “you don’t sound wheezy” can feel like a denial of your lived reality.
-
Loss of role – Illness can mean stepping back from work, family responsibilities, or social life, leaving you feeling less “you” and more “the patient.”
2. The Healthy Person’s Perspective
Even the most loving partner, friend, or family member has finite emotional reserves:
-
Empathy fatigue – Offering compassion in a crisis is natural; sustaining it daily for years is emotionally exhausting.
-
Positivity limits – Staying upbeat to encourage the patient can drain energy, sometimes leading to withdrawal.
-
Healthy guilt – Feeling bad for having health, energy, freedom, or the ability to enjoy life.
-
Emotional self-protection – Avoiding deep illness discussions to manage their own fear, helplessness, or sadness.
-
Mismatch of experience – The healthy person dips in and out of illness awareness, while the patient lives in it constantly.
3. Patient Guilt
While healthy guilt is common, patient guilt is just as powerful:
-
Feeling like a burden – Worrying that you limit others’ activities, social life, or freedom.
-
Changing the relationship – Feeling bad that a partner now has to act partly as a carer.
-
Financial strain – Guilt over reduced income or increased expenses.
-
Impact on others’ wellbeing – Feeling responsible for your partner’s, friends’, or family’s stress or fatigue.
-
Mood and personality changes – Guilt about being irritable, anxious, or withdrawn because of the illness or medication effects.
4. Common Relationship Challenges
For partners:
-
Role shift – Moving from equal partnership to a dynamic where one is part-carer.
-
Social imbalance – One may want to go out more than the other can manage.
-
Resentment risk – If needs are unspoken, one may feel abandoned and the other may feel trapped.
For family:
-
Unequal support – Some relatives engage, others withdraw.
-
Generational differences – Older relatives may minimise invisible illness (“just push through”).
-
Positive minimising – Trying to “cheer you up” by downplaying symptoms, which can feel invalidating.
For friends:
-
Friendship drift – Reduced shared activities can lead to less contact.
-
Fear of offending – Friends stop inviting you to events so you won’t have to say no.
-
Discomfort with illness – Some disappear entirely rather than risk awkwardness.
5. The Psychology Behind These Changes
-
Finite empathy and energy – The brain isn’t wired for sustained crisis-mode support.
-
Visible vs. invisible illness gap – We respond more readily to what we can see (limping, coughing) than what we can’t (chest tightness, fatigue).
-
Avoidance coping – Healthy people sometimes step back emotionally to manage their own distress.
-
Healthy guilt – Creates distance when the healthy person hides their joy to avoid hurting you.
-
Patient guilt – Creates distance when you hold back your needs to avoid burdening them.
6. Strategies for Moving Forward Together
For Patients:
-
Be specific – Say what you need: “I need you to just listen” or “Could you help with…?”
-
Make space for non-illness moments – Talk about hobbies, TV shows, shared memories.
-
Recognise recharge needs – Allow healthy people breaks from illness talk without taking it as a lack of care.
-
Value their life too – Encourage them to enjoy activities even if you can’t join.
For Partners, Friends, and Family:
-
Believe them – Accept what the patient says about symptoms, even if they “look fine.”
-
Share your feelings – Guilt, overwhelm, or fear are normal; discussing them prevents silent withdrawal.
-
Keep inviting – Offer options, but no pressure — inclusion matters more than attendance.
-
Balance care with normality – Don’t let every interaction be about the illness.
7. Talking About Guilt (Both Sides)
-
Name it openly – “I feel guilty for being well” or “I feel guilty for needing so much help.”
-
Acknowledge the illness isn’t anyone’s choice – Blame the condition, not each other.
-
Agree on boundaries – Both lives matter, both deserve joy.
-
Share in two directions – Illness updates and everyday life keep relationships in balance.
8. Final Thought
Chronic illness can strain relationships, but it can also deepen them — if both sides:
-
Understand that empathy, positivity, and energy are finite.
-
Recognise both healthy guilt and patient guilt.
-
Protect space for joy, humour, and connection beyond the illness.
Love doesn’t mean living in the illness 24/7 — it means walking alongside each other, even when the paths look different.

Information on Allergic BronchoPulmonary Aspergillosis (ABPA) / SAFS – For Family and Friends
Print out or share electronically
WHAT IT IS
ABPA (Allergic Bronchopulmonary Aspergillosis) and SAFS (Severe Asthma with Fungal Sensitisation) are allergic reactions to a common fungus, Aspergillus. In some people with asthma, the immune system overreacts to spores in the air, causing inflammation, swelling, and mucus plugs in the lungs.
WHAT IT'S NOT
-
Not contagious – you can't catch it.
-
Not poor hygiene – Aspergillus is everywhere in the air.
-
Not the patient's fault – flare-ups happen because of the condition, not something they did or didn't do.
WHY AREN'T OTHERS AFFECTED?
Most people's lungs clear these spores easily. In ABPA/SAFS the immune system reacts too strongly – more likely with long-standing asthma, severe allergies, damaged airways (e.g., bronchiectasis), or a genetic tendency. It's not weakness or lifestyle choices – often just lung history and bad luck.
TYPICAL SYMPTOMS
-
Wheezing, cough (sometimes with mucus plugs)
-
Breathlessness
-
Severe fatigue
-
Sometimes coughing up blood
WORST SYMPTOMS
-
Mucus plugs – thick, sticky clumps blocking airways, making breathing suddenly harder.
-
Intense coughing – can be exhausting, cause chest pain, and disrupt sleep.
TREATMENT
-
Anti-inflammatory medicines (often steroids)
-
Antifungals to reduce Aspergillus in the airways
-
Biologics for severe asthma/allergic inflammation
-
Monitoring with blood tests, breathing tests, and scans
THE REALITY
This condition can dominate daily life. On bad days the person may not be able to do much at all. Energy and breathing can change day-to-day (even hour-to-hour). If plans are cancelled, it isn't a lack of interest – it's the illness. Flare-ups can also make people feel short-tempered – a natural reaction to frustration, not a lack of care. Many people also live with a constant awareness of environmental risks – weighing up every new place or activity for dust, damp, or spores. This can feel exhausting and may lead them to avoid situations that others wouldn’t think twice about.
LOOKING AHEAD
-
With good control – Many people manage their symptoms well, reduce flare-ups, and keep active with the right treatment and avoidance of triggers.
-
Risks – Without good control, repeated flare-ups can slowly damage the lungs and lead to bronchiectasis.
-
Change over time – Some improve and need less treatment; others have ongoing ups and downs. Early action on flare-ups makes a big difference.
ENVIRONMENTAL TRIGGERS & PROTECTION
Some people with ABPA or SAFS have to avoid dust, mould, strong smells, smoke, and damp places – these can trigger flare-ups. Activities like gardening, compost turning, or DIY can be risky because they release fungal spores into the air. Wearing a well-fitting mask (e.g., FFP2/FFP3) can help reduce exposure – it's about staying well, not being antisocial.
HOW FRIENDS AND FAMILY CAN BEST HELP
-
Be flexible with plans – energy and breathing can change suddenly; last-minute cancellations aren't personal.
-
Help avoid triggers – choose low-dust, low-mould venues and activities.
-
Support treatment routines – lifts to appointments, collecting prescriptions, or reminders if welcome.
-
Listen without judgement – let them share symptoms and frustrations.
-
Encourage safe activities – suggest hobbies and outings with low environmental risk.
-
Show affection and reassurance – a hug, a kind message, or checking in can mean a lot.
MORE INFORMATION & SUPPORT
National Aspergillosis Centre (UK): https://mft.nhs.uk/wythenshawe/services/infectious-diseases/national-aspergillosis-centre/
Patient information & community: https://aspergillosis.org

Chronic Pulmonary Aspergillosis (CPA) – Information For Family and Friends
Print this off or share electronically
WHAT IT IS
CPA (Chronic Pulmonary Aspergillosis) is a long-term lung infection caused by the Aspergillus fungus. It often develops where lungs are already damaged (e.g., TB, COPD, bronchiectasis, sarcoidosis) and may form cavities, sometimes with fungal balls (aspergillomas).
WHAT IT'S NOT
-
Not contagious – you can't catch CPA.
-
Not poor hygiene – spores are everywhere in the air.
-
Not the patient's fault – flare-ups or setbacks happen because of the illness, not something they did wrong.
WHY AREN'T OTHERS AFFECTED?
Most people remove spores without trouble. CPA appears when lungs are already damaged or the immune system can't fight the fungus well – after past infections, chronic lung disease, or weakened defences. It's not about choices; it's lung history and chance.
TYPICAL SYMPTOMS
-
Persistent cough (sometimes with blood)
-
Breathlessness
-
Fatigue and low energy
-
Weight loss
-
Recurring chest infections
WORST SYMPTOMS
-
Coughing up blood – can be small streaks or larger amounts; sudden and frightening; urgent if heavy.
-
Severe fatigue – can stop even simple tasks; not just ‘tiredness’.
TREATMENT
-
Long-term antifungal medication
-
Regular scans and blood tests
-
Surgery in selected cases
THE REALITY
CPA is a serious, long-term condition. On bad days, people may not be able to do much at all. Symptoms can dominate daily life and limit social plans – cancelled arrangements are the illness talking, not them. It can also make people feel grumpy or irritable – not because they don't care, but because constant symptoms, tiredness, and limits on daily life are frustrating and exhausting. There’s often a mental load too – always thinking about avoiding dust, damp, or mould spores, and sometimes feeling overcautious about activities like going on boats, visiting old buildings, or anywhere that might harbour moisture or mould. This risk-checking is a form of self-protection, even if it means missing out.
It’s important to mention the mood swings and fatigue caused not only by the disease but also by the medication. For some, constant hand tremors are also part of daily life — these are often misunderstood by others.
LOOKING AHEAD
-
With effective treatment – Many people can keep the infection stable for years, control symptoms, and stay independent.
-
Risks – CPA can slowly progress, and severe flare-ups (like coughing large amounts of blood) may need urgent treatment.
-
Change over time – The illness can be stable for long periods, but it often needs lifelong monitoring and treatment changes. Support from specialists helps keep people well for longer.
ENVIRONMENTAL TRIGGERS & PROTECTION
Some people with CPA need to avoid environments with high levels of dust or fungal spores. This includes gardening, composting, building work, or damp/mouldy places. Wearing a protective mask during these activities can help reduce risk. Avoiding these triggers is about preserving lung health – not being fussy or antisocial.
HOW FRIENDS AND FAMILY CAN BEST HELP
-
Respect limits – breathlessness, fatigue, or coughing up blood can stop plans at short notice; it's not a choice.
-
Minimise exposure risks – avoid inviting them to dusty, damp, or mouldy places.
-
Offer practical help – driving to appointments, carrying shopping, or helping at home during flare-ups.
-
Be patient with mood changes – grumpiness can come from exhaustion and constant vigilance against triggers.
-
Talk openly about safety – if you suggest an outing, ask “Would this feel safe for you?”
-
Stay connected – even if they can't join in physically, a call or small gesture keeps them included.
MORE INFORMATION & SUPPORT
National Aspergillosis Centre (UK): https://mft.nhs.uk/wythenshawe/services/infectious-diseases/national-aspergillosis-centre/
Patient information & community: https://aspergillosis.org

Damp, Cold, and Poor Housing – Why It Matters for Lung Health
This briefing from the House of Commons Library (2025) looks at how poor housing conditions—especially damp, mould, and cold homes—affect health and what’s being done about it in the UK.
Main Points
-
Health risks are serious
Living in damp or mouldy homes increases the risk of respiratory problems, particularly for people with existing lung disease like aspergillosis, asthma, COPD, or bronchiectasis. -
Children and vulnerable adults
Young children, older adults, and people with weakened immune systems are most affected. Damp and mould can trigger flare-ups, worsen breathing symptoms, and increase infection risk. -
Mental health impact
Poor housing is linked to stress, anxiety, and depression. Worrying about your home can also worsen physical symptoms, especially if you avoid using rooms with mould or limit heating to save costs. -
Cold homes add to the problem
Cold airways can make breathing more difficult, weaken the immune system, and increase the chance of winter infections. -
Wider health effects
Damp and cold can also affect heart health, bone/joint pain, and overall wellbeing.
What’s Being Done
-
Legal responsibilities: Landlords must keep homes safe and fit to live in under UK law. This includes dealing with serious damp and mould.
-
Government programmes:
-
Funding for improving insulation and heating in social housing.
-
Advice services for tenants.
-
Local councils can take action if landlords fail to address hazards.
-
-
Public health guidance now recognises the link between housing and chronic illness, with stronger advice for early intervention.
What This Means for Aspergillosis Patients
-
Stay alert to symptoms: If your cough, breathlessness, or fatigue worsen at home, check for damp, mould, or poor heating.
-
Act early: Report problems to your landlord or council quickly—prolonged exposure can worsen lung damage.
-
Medical link is recognised: You are more likely to be taken seriously now, as official guidance acknowledges the health risks.
-
Keep records: Photos, symptom diaries, and GP notes can support housing complaints.
For full details see https://commonslibrary.parliament.uk/research-briefings/cdp-2025-0096/
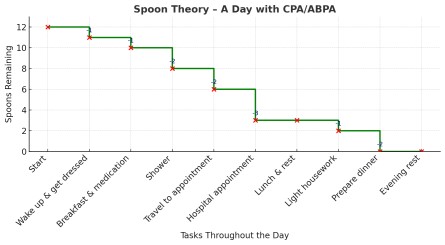
Spoon Theory: Making Sense of Energy Limits in Aspergillosis
The Spoon Theory is a way of explaining what it’s like to live with a long-term illness that affects your energy and stamina. It was first described by Christine Miserandino, who used spoons as a visual metaphor for the limited amount of energy she had each day.
How it works
-
Imagine you start each day with a set number of spoons — maybe 10 or 12.
-
Every task you do “costs” spoons:
-
Getting dressed might cost 1 spoon
-
Cooking a meal might cost 2 spoons
-
A shower could cost 2 spoons on a bad day
-
Going for a walk or attending an appointment might cost 3 or 4 spoons
-
-
When you run out of spoons, that’s it — you don’t have the energy to keep going. If you push yourself, you “borrow” from tomorrow’s spoons, which can leave you feeling worse for days.
 Why CPA and ABPA drain your spoons
Why CPA and ABPA drain your spoons
 Why CPA and ABPA drain your spoons
Why CPA and ABPA drain your spoonsBoth conditions can cause:
-
Breathlessness – even small tasks can feel like hard work.
-
Coughing and mucus production – which can be exhausting physically.
-
Flare-ups – like haemoptysis (coughing blood) in CPA or allergic inflammation in ABPA.
-
Medication side effects – antifungals, steroids, or biologics can also sap your energy.
-
Frequent appointments – travel and hospital visits can eat into your spoon supply.
Why Spoon Theory matters
Understanding Spoon Theory helps you:
-
Plan your day – save enough spoons for the important things.
-
Pace yourself – spread out demanding tasks, rest between them.
-
Explain your limits – it’s an easy way to help friends, family, and employers understand that you’re not being lazy — you’re managing your limited energy.
-
Avoid “boom and bust” – pushing too hard on a good day can leave you with no spoons for the next few days.
Practical tips
-
Prioritise – decide what’s essential today and what can wait.
-
Ask for help – let others “spend” their spoons for you when possible.
-
Rest without guilt – recharging is part of living with a long-term condition.
-
Track your spoons – keeping a symptom diary can help you notice patterns.
Remember: Your number of spoons can change day-to-day, especially if you’ve had a flare-up, infection, or a hospital stay. Learning to work with your spoons instead of against them can help you stay in control and reduce stress.