
Working With Your Medical Team: What Every Patient With Aspergillosis Needs to Know
Modern antifungal treatments, and many of the medicines used alongside them, can be life-saving. They help control infections that would otherwise cause severe damage to the lungs and other organs. But these medicines are also powerful, and like all strong treatments, they sometimes carry risks.
One patient recently shared that they developed nerve damage (neuropathy) while taking antifungal medication, but did not mention it to their doctor because they did not know it could be a side effect. Sadly, problems like this can sometimes become permanent if not spotted early.
This raises an important question: what do patients need to know about their responsibilities when taking medicines like antifungals, and more broadly, when living with aspergillosis?
From passive role to partnership
In the past, healthcare often worked in one direction: the doctor gave instructions, and the patient was expected to follow them. Patients were mostly passive, with little chance to ask questions or take part in decisions.
The NHS is now moving towards a very different way of working: partnership.
This means:
-
Doctors and nurses share their medical knowledge.
-
Patients share their experiences of living with their condition.
-
Together, both sides decide what treatment and care will work best.
Why doctors sometimes hesitate about side effects
Some patients are surprised to learn that not all doctors automatically tell patients about possible side effects. Why is this?
-
Some worry about causing anxiety or putting patients off treatment.
-
Others fear the nocebo effect — where simply knowing about a side effect can make someone more likely to notice it.
-
They may also feel that handing over a long list of possible effects is overwhelming.
But when it comes to antifungals and other long-term, powerful medicines, not knowing can be dangerous. If patients do not know what to look for, they may ignore early signs of serious problems until it is too late.
The best approach is balance:
-
Patients don’t need to memorise an endless list.
-
They do need a clear, short list of the most important and urgent symptoms to look out for — and to know what to do if they appear.
Medicines: what patients should do
-
Take medicines as prescribed – antifungals, inhalers, steroids, or biologics must be taken on schedule. Missing doses can reduce effectiveness or drive resistance.
-
Do not stop suddenly – especially steroids. Always follow tapering advice.
-
Check for interactions – antifungals can clash with common medicines such as statins, blood pressure tablets, and painkillers. Always tell your team about new prescriptions, over-the-counter drugs, or supplements.
-
Use the same pharmacy if possible – so interactions are checked consistently.
Monitoring your health
-
Attend all scheduled tests – blood work, lung function, CT scans. These can reveal hidden changes before you feel them.
-
Know your “normal” – keep track of oxygen levels (if you use a pulse oximeter), peak flow, sputum colour, cough, and breathlessness.
-
Spot infections early – worsening cough, fever, or new sputum colour may mean infection or flare-up. Report these quickly.
Communication with your team
-
Bring notes to clinic – write down questions and symptoms so nothing is forgotten.
-
Be open and honest – if you’ve missed doses, struggled with side effects, or found treatment difficult, let your team know.
-
Keep contact details handy – know who to call if problems arise (specialist nurse, hospital helpline, GP).
Lifestyle and prevention
-
Reduce exposure to moulds – avoid compost heaps, rotting leaves, damp basements, and building dust. If you cannot avoid them, wear an FFP2/3 mask.
-
Protect your lungs – keep up with vaccinations (flu, COVID-19, pneumococcal).
-
Support your overall health – eat well, stay as active as you can, and rest when needed.
-
Look after your mental health – chronic illness is stressful. Patient groups, counselling, or peer support can make a big difference.
Self-management skills
-
Recognise flare-ups – learn the difference between ABPA flare, CPA progression, and bacterial infection symptoms.
-
Know your rescue plan – what to do if you suddenly worsen (extra inhalers, antibiotics, or emergency help).
-
Keep records – note symptoms, hospital visits, and medication changes. This helps spot long-term patterns.
-
Be part of decisions – ask about benefits, risks, and alternatives of treatments. Care should fit your life as well as your lungs.
Where to find reliable information on medicines
Many patients say the leaflet in the medicine box is written in tiny print or feels overwhelming. You do have other options:
-
Ask your clinical team or pharmacist — they can give you a short list of the most important side effects to watch for and explain what’s urgent.
-
Check the BNF (British National Formulary) online — the NHS makes this trusted reference free to the public at bnf.nice.org.uk. It lists side effects, drug:drug interactions, and safety notes.
-
Use NHS.uk — clear pages on most medicines, written in plain English.
-
Patient support organisations — such as the National Aspergillosis Centre or relevant charities, which often provide tailored advice.
If you’re unsure, it’s always safer to ask rather than guess.
The bigger picture: partnership
In the past, doctors made decisions and patients followed instructions. Today, with complex conditions like aspergillosis, patients are central members of the care team.
-
You notice problems first.
-
You take daily responsibility for medication.
-
You decide when to seek help.
This isn’t about shifting the whole burden onto patients — it’s about recognising that care works best when it is a true partnership.
Key message
👉 If you notice something new, strange, or worrying while on antifungal medication — however small — tell your healthcare team. Don’t assume it’s not important.
And remember: safe, effective treatment is a two-way street. Your role as a patient is not just to take medicines, but to observe, record, communicate, and partner with your team. That partnership is what keeps you safe and makes your treatment work.
👩⚕️ Martha’s Law – What It Means for Aspergillosis Patients
Why the law was introduced
-
Martha Mills was a 13-year-old girl who died in 2021 after developing sepsis in hospital.
-
Her parents felt their concerns were not acted on quickly enough and that they were not given access to a second opinion.
-
In response, the government announced Martha’s Law, to ensure patients and families can easily get a second clinical opinion if they feel their concerns are not being taken seriously.
What the law requires
-
Hospitals must provide a clear and simple process for patients and families to request a second opinion from a senior doctor.
-
This right applies when someone feels that:
-
Their symptoms are worsening or not being managed properly.
-
They are not being listened to by the care team.
-
They need reassurance that their treatment plan is the right one.
-
-
Staff must also inform patients and carers about this right so people know it is available.
Why this matters for people with Aspergillosis
-
Aspergillosis is a rare and complex condition, and not all hospitals or clinicians have specialist knowledge.
-
Symptoms (e.g. breathlessness, chest pain, fever, wheeze, coughing blood) can be misinterpreted as asthma, pneumonia, or something less serious.
-
Martha’s Law means that if you or your family feel your care isn’t right, you can:
-
Request a second opinion promptly.
-
Be assessed by another senior doctor, potentially with respiratory or infectious disease expertise.
-
Gain access to the National Aspergillosis Centre or another specialist service if appropriate.
-
What you can do if concerned
-
Speak up early: tell staff if you are worried about your symptoms getting worse.
-
Ask for a second opinion: mention “Martha’s Law” if you feel you’re not being heard.
-
Bring your information: if you’re an aspergillosis patient, carry your clinic letters or patient passport to help new doctors understand your condition.
-
Involve carers/family: they can raise concerns on your behalf if you are too unwell.
✅ In summary: Martha’s Law ensures that patients and families have the right to be heard and to request a second medical opinion. For people with aspergillosis, this could be life-saving when symptoms are worsening and urgent, specialist input is needed.
Housing Reforms That Matter for Aspergillosis Patients
1. Awaab’s Law – Protecting Against Damp & Mould
-
Born from the tragic death of toddler Awaab Ishak, Awaab’s Law mandates swift action on damp and mould in social housing.
-
Phase 1 (from 27 October 2025):
-
Emergency hazards addressed within 24 hours.
-
Investigations into mould/damp begin within 10 working days.
-
Findings communicated within 3 working days.
-
Repairs completed within 5 working days, with alternative housing offered if unsafe.
Chartered Institute of HousingGOV.UK
-
For aspergillosis patients, this delivers critical protection—damp environments exacerbate lung disease, and timely remediation can make a real health difference.
2. Decent Homes Standard (DHS) – Public Consultation Open
The government is reviewing and expanding the Decent Homes Standard to include both social and private rented sectors.
-
Consultation open 2 July to 10 September 2025.
-
New proposals include:
-
A firm requirement for homes to be free from damp and mould.
-
Updating standards around heating, insulation, window security, flooring, and accessibility.
GOV.UKconsult.communities.gov.ukNorthern Housing Consortium
-
Why this matters for you: Contributing your experiences—especially how damp or poor insulation worsen aspergillosis—can help shape a standard that better protects lung health.
3. Electrical Safety Regulations for Social Landlords
-
From November 2025 (new tenancies) and May 2026 (existing tenancies), social landlords must:
-
Perform electrical safety checks (EICR) every five years.
-
Supply tenants or new occupants with the inspection report within 28 days.
-
Conduct Portable Appliance Testing (PAT) and fix any hazards within 28 days.
GOV.UKTrowers & Hamlins
-
Why it matters: Safe electrics reduce the risk of fires and power outages, which can be particularly dangerous during respiratory flare-ups or hospital recovery.
4. Other Related Reforms & Building Safety Measures
-
Gas Safety: Landlords must continue annual checks of gas appliances and provide tenants with a valid Gas Safety Certificate (CP12).
Wikipedia -
Building Safety Act & Regulations (Part P): Ensures electrical work (like rewiring or EV charger installations) meets safety standards—crucial for safe, modern living environments.
HomebuildingWikipedia -
Energy Efficiency Reforms: Proposals (not yet enacted) suggest requiring rented homes to reach a C rating on Energy Performance Certificates (EPC) by 2030 to reduce fuel poverty and keep homes warm.
The TimesThe Guardian
Summary Table
| Reform / Law | Scope & Timing | Why It Matters for Aspergillosis Patients |
|---|---|---|
| Awaab’s Law – Phase 1 | From 27 Oct 2025 | Ensures damp/mould issues are addressed fast |
| Decent Homes Standard Consultation | 2 Jul – 10 Sep 2025 | Influences future standards to protect lung health |
| Electrical Safety Regulations | From Nov 2025 / May 2026 (depending on tenancy) | Mitigates fire/electrical risks in homes |
| Gas Safety Standards | Ongoing requirement | Prevents gas-related hazards in vulnerable patients |
| Building Safety & Part P Rules | Already in effect | Ensures electrical works meet safety compliance |
| Energy Efficiency Initiatives | Proposed for 2030+ | Promotes warm, dry living conditions |
What You Can Do
-
Submit to the DHS consultation by 10 September, sharing your stories of how damp or poor heating affects your lung health.
-
Report damp or mould to your landlord and ask for Awaab’s Law protections—mention the upcoming deadlines.
-
Ensure safety checks are done—ask your landlord for the EICR or gas safety certificate.
-
Highlight your needs—if you have aspergillosis, a doctor’s note can underline the urgency for timely action.
Would you like help drafting a consultation response template or patient-facing summary sheet to guide people through these updates? Just let me know!

The Times

National Aspergillosis Centre Video Recordings

NAC Monthly Patient Meetings
The NAC monthly patient meetings provide a friendly, supportive, and informative space for anyone living with aspergillosis or related conditions. Hosted by the National Aspergillosis Centre (NAC), these sessions bring together patients, carers, and healthcare professionals to:
-
share personal experiences
-
ask questions in a safe environment
-
hear the latest updates on treatments, research, and self-care strategies
🎥 Watch past sessions
Our YouTube channel now has 87 recordings, covering everything from expert talks to personal patient stories. Whatever your stage in the journey — newly diagnosed or managing your condition for years — you’ll find something helpful and relatable.
Recent Highlights
-
September — Explored how Artificial Intelligence can support patients in finding trustworthy information. We also answered community questions about biologic medications, looking at what research tells us about their long-term effectiveness in asthma and ABPA.
-
August — Focused on new biologics for severe asthma, discussing why they don’t always work for everyone, and why some patients see benefits fade over time.
-
July — Shared updates from the British Thoracic Society meeting in Manchester, plus further insights into what the future may hold for biologic treatments.
💡 Whether you want practical advice, the latest medical updates, or simply the chance to connect with others who truly understand your journey, the NAC monthly meetings are here for you.

🧑🤝🧑 Taking Part in Your Own Care: Shared Decision-Making, Self-Management & Advocacy in the NHS
Living with a long-term condition like aspergillosis can be complicated. You may see hospital specialists, your GP, nurses, pharmacists, and sometimes social services too. The NHS is working hard to make sure patients aren’t just “done to,” but are real partners in decisions about their own health.
This approach is called shared decision-making and supported self-management.
🌱 Where did this idea come from?
-
It’s a core part of the NHS Long Term Plan (2019, refreshed 2023/24).
-
The aim: give patients a stronger voice, improve care outside hospital, and reduce emergency admissions.
-
It grew out of earlier “shared care” models, where GPs and hospitals split prescribing or monitoring tasks. Now the focus is much wider: putting patients at the centre of their own care.
💡 What does it mean?
Shared decision-making
-
You and your clinicians decide together.
-
Doctors explain the evidence, options, risks, and benefits.
-
You share what matters most to you — daily life, family, work, fears, and preferences.
-
Example: deciding whether to start biologics, taper steroids, or continue antifungal therapy.
Self-management
-
You are supported to handle your condition day-to-day.
-
This includes recognising early warning signs, having an action plan, knowing when to call for help, and using tools like the NHS App or support groups.
-
Education, pulmonary rehab, peer groups, and digital health apps can all help.
🚧 Barriers patients may face
Even though the NHS wants all patients involved in their care, challenges exist:
-
Short appointments that leave little time for discussion.
-
Medical jargon that is hard to follow.
-
Confidence gaps, especially when you feel unwell.
-
Health inequalities (literacy, language, digital access).
-
Fragmented care, where GP and hospital don’t always join up.
-
Information overload — too much general advice, not enough personalised guidance.
🧑🤝🧑 Can you have an advocate?
Yes. You don’t have to face this alone. Advocacy can come from:
-
Specialist nurses at the National Aspergillosis Centre (NAC) or your local hospital.
-
Family or friends — you are always entitled to bring someone to appointments.
-
Peer groups like NAC CARES, where other patients share practical advice.
-
PALS (Patient Advice and Liaison Service) in every NHS trust.
-
Healthwatch (local branches) or independent advocacy charities.
🔎 Care Coordinators & Link Workers
These are newer NHS roles that help patients navigate complex care.
Care coordinators
-
Support people with complex, long-term conditions.
-
Help organise appointments, blood tests, and follow-up.
-
Make sure GPs, hospitals, and community services talk to each other.
-
Often based in Primary Care Networks (PCNs) or specialist hospital clinics.
Social prescribing link workers
-
Focus on the non-medical side of health.
-
Connect patients to local community support, peer groups, exercise schemes, benefits advice, or housing help.
-
Anyone struggling with isolation, anxiety, or lifestyle issues can be referred.
📋 Criteria for Accessing Care Coordinators & Link Workers
Care Coordinators – who qualifies?
-
Patients with two or more long-term conditions, or one condition requiring complex management (e.g. aspergillosis with antifungals, steroids, biologics, adrenal monitoring).
-
People on multiple medicines or with frequent hospital admissions.
-
Patients needing help to coordinate care between GP, hospital, pharmacy, and community services.
-
Prioritised for those at risk of “falling through the cracks” in the system.
Social Prescribing Link Workers – who qualifies?
-
Any patient whose social or practical situation affects their health.
-
Examples:
-
Feeling isolated or low in mood.
-
Struggling with benefits, housing, or finances.
-
Wanting help with lifestyle changes.
-
Needing connections to peer groups or local activities.
-
-
Usually no strict medical criteria — referral is based on need.
How referrals usually happen
-
GP or practice nurse refers after spotting a need.
-
Hospital team (e.g. NAC or respiratory clinic) may suggest referral back to the GP/PCN.
-
Some PCNs allow self-referral if the service is advertised locally.
📊 How many coordinators are there?
-
As of mid-2025, NHS England data shows:
-
Around 5,000–6,800 full-time equivalent care coordinators employed across Primary Care Networks.
-
Over 3,500 social prescribing link workers active across England.
-
-
Numbers vary by area, and coverage is still expanding as ICSs and PCNs grow their teams.
🧠 Why do people think care coordination is mostly mental health?
-
Historically, most care coordinators were employed in mental health services, where patients often need joined-up support from psychiatry, GPs, housing, benefits, and social care.
-
That’s why many people first hear the term “care coordinator” in relation to community mental health teams.
-
But the NHS is now expanding care coordination into physical long-term conditions, including respiratory diseases like COPD, bronchiectasis, and aspergillosis.
-
Access still varies by region — some areas prioritise cancer, frailty, or diabetes, while others are starting to include respiratory patients.
🧑⚕️ Care Coordination: Mental Health vs Physical Health
| Aspect | Mental Health (traditional focus) | Physical Health (expanding role) |
|---|---|---|
| Where based | Community Mental Health Teams | Primary Care Networks (GP groups), hospital specialist clinics |
| Why developed | To join up psychiatry, GPs, social care, housing, and benefits | To support patients with multiple long-term conditions (e.g. COPD, diabetes, aspergillosis) |
| Patient needs | Severe mental illness, complex social problems, frequent crisis episodes | Complex care plans, multiple medicines, hospital visits, difficulty managing appointments |
| Tasks | Coordinate mental health reviews, social support, community referrals | Organise tests and follow-ups, link GP and hospital, ensure medication and monitoring plans are clear |
| Referrals | Usually from psychiatrist or community mental health nurse | Usually from GP practice, sometimes via hospital specialist or self-referral in PCN areas |
| Examples | Patient with schizophrenia needing GP, psychiatrist, housing officer all linked | Patient with aspergillosis on antifungals, steroids, and biologics needing joined-up GP + hospital care |
| Extra support | Peer groups, advocacy, PALS, housing officers | Social prescribing link workers, community health support, peer groups (e.g. NAC CARES) |
✅ What this means for aspergillosis patients
-
If you have complex care needs (antifungal monitoring, biologics, steroid side-effects, adrenal insufficiency, other chronic conditions), you are likely to meet criteria for a care coordinator.
-
If you are struggling with the social and emotional impact of illness (fatigue, isolation, money worries, lifestyle changes), you may benefit from a link worker.
-
These roles are increasingly available in GP networks, though availability may differ locally.
-
Ask both your hospital team and your GP practice what is available in your area.
🔍 Questions to ask at your next appointment
-
Could I be referred to a care coordinator to help manage my appointments and medicines?
-
Is there a link worker who can support me with non-medical needs?
-
What local services are available through my Primary Care Network or ICS?
-
Who is responsible for updating my care plan?
-
What support is there for my carer or family?
💬 In summary:
Shared decision-making and self-management mean you are an active partner in your care. Aspergillosis is complex, but you don’t have to manage it alone. Between your hospital specialists, GP, advocates, and newer NHS roles like care coordinators and link workers, there is growing support available across the NHS to help you live better and feel more in control.
⚠️ Mistakes in NHS Care: Why They Happen & What You Can Do
🔎 Why mistakes happen
-
Heavy workload: Doctors and nurses handle huge numbers of patients and results every day.
-
Fragmented IT systems: GP, hospital, and lab systems don’t always link, so information can get lost.
-
Human error: Fatigue, multitasking, and assumptions all increase the risk of oversight.
-
Defensive culture: Trusts sometimes minimise problems to protect reputation or avoid litigation.
Most errors are not deliberate — but they can cause harm if they are not caught quickly.
Martha’s Rule was created after a young girl died when her family’s concerns were ignored — it’s designed to stop that happening again.
🛡 What safeguards are already in place?
Although mistakes still happen, the NHS has many systems to reduce risk and catch errors early:
-
Critical results alerts: Labs automatically flag dangerously abnormal results so they cannot be overlooked.
-
Early Warning Scores (NEWS2): Vital signs generate a score that prompts urgent review if the patient is deteriorating.
-
Sepsis protocols: Hospitals have rapid-response pathways for suspected sepsis.
-
Cross-checking: High-risk drugs often require two professionals to sign off.
-
Incident reporting: Staff can log “near misses” to help the system learn.
-
Duty of Candour: Trusts must inform patients if serious harm has been caused by an error.
-
Martha’s Rule: Gives patients/families the right to request an urgent independent review if they feel concerns are being ignored.
💻 Are new IT systems making care safer?
The NHS is moving to large electronic patient record (EPR) systems such as Epic, Cerner and Lorenzo. These bring real safety gains:
Safer features
-
Automatic alerts for critical blood results.
-
Built-in early warning score (NEWS2) calculations to detect deterioration.
-
Electronic prescribing with dose, allergy, and interaction checks.
-
Shared records across hospitals, GPs, and community services.
-
Digital audit trails showing who reviewed results and when.
But challenges remain
-
Too many alerts can cause “alert fatigue,” leading staff to dismiss warnings.
-
System crashes or downtime can force staff back to paper, which is less safe.
-
Complexity can slow clinicians down until they are confident with the system.
-
Hospital and GP systems still don’t fully integrate everywhere, so results can still be missed.
Bottom line: New IT has improved safety compared to the old paper-and-fax systems, but it isn’t foolproof. It works best alongside clinical vigilance and patient involvement.
✅ What you can do if you suspect a mistake
Step 1. Check directly with the clinical team
-
Ask: “Can you confirm this result/issue has been reviewed?”
-
Request a written explanation or clinic letter.
-
Keep notes of the conversation.
Step 2. Escalate to a senior doctor/clinical lead
-
Ask who the consultant in charge is.
-
Write your concern clearly and factually.
Step 3. If your loved one is deteriorating: use Martha’s Rule
-
You can request an urgent review by a critical care team, separate from the ward team.
-
Available 24/7 in hospitals where introduced.
-
Say: 👉 “We want a review under Martha’s Rule.”
-
If not yet in your hospital, ask for the critical care outreach team.
Step 4. Contact PALS (Patient Advice & Liaison Service)
-
They can chase answers and log concerns.
Step 5. Make a formal complaint to the Trust
-
Keep it factual (what happened, why it matters, what outcome you want).
-
The Trust must acknowledge within 3 working days.
Step 6. Escalate outside the Trust
-
If unsatisfied, go to the Parliamentary and Health Service Ombudsman (PHSO).
🧭 Tips to protect yourself & your family
-
Keep copies of all results and letters.
-
Track your results in a simple log.
-
Bring support (family, advocate, charity like AvMA).
-
Stay factual: stick to dates, facts, and impact.
🔑 Key message
Mistakes in healthcare happen for many reasons — but the NHS has safeguards and new IT systems to reduce risk, and Martha’s Rule adds an extra urgent safety net.
Patients and families still play a vital role by asking questions, checking results, and speaking up.
You are not being difficult — you are being safe.
Misinformation on Social Media: Health and Beyond
Social media helps us stay connected, share experiences, and find support. But it also spreads false or misleading stories — about health, politics, money, and world events. These stories can cause unnecessary fear, confusion, and sometimes real harm if people act on them.
Understanding why misinformation spreads, what’s being done about it, and how to spot it helps keep you and your loved ones safe.
🚩 Why do false stories spread?
-
Algorithms reward attention
Platforms are designed to keep you scrolling. Content that shocks (“miracle cure discovered!”), scares (“hidden danger you’re not being told about!”), or excites spreads the fastest — even if it isn’t true. -
Anyone can post anything
Unlike newspapers, medical journals, or BBC/NHS websites, most social media posts aren’t checked by editors or experts before going live. -
Echo chambers
Platforms show you more of what you already click on. If you read about miracle diets or political conspiracies, you’ll see more of them — true or not. -
Deliberate misinformation
Some people spread falsehoods deliberately:-
To sell fake health products
-
To make money from clicks
-
To influence politics or sow division
-
-
Speed beats accuracy
False stories can go viral in minutes. Corrections are slower and rarely reach as many people.
⚖️ What’s being done about it?
Legal approaches
-
UK: The Online Safety Act (2023) requires platforms to remove illegal or harmful misinformation, including dangerous health advice.
-
EU: The Digital Services Act (DSA) makes large platforms responsible for acting faster against harmful content.
-
Extreme cases: Fraud, scams, defamation, or incitement of violence are not protected speech and can be prosecuted.
Technical approaches
-
Algorithms: AI flags suspicious posts.
-
Labelling: Content can be marked as “false” or “missing context.”
-
Bot control: Platforms limit fake accounts that spread stories at scale.
-
Digital nudges: Some apps ask “Do you want to read before sharing?” or warn if a post is outdated.
The limits
-
Freedom of speech protects many misleading opinions unless they cause direct harm.
-
Global reach makes it hard to police.
-
Volume — billions of posts daily are impossible to check one by one.
-
Trust — some people ignore fact-check labels, believing platforms are biased.
🧐 How to know what’s real
Five quick checks:
-
Who is posting it? NHS, WHO, BBC, or Reuters → reliable. Unknown influencer or “miracle cure” shop → beware.
-
Is it reported elsewhere? Real news appears in multiple reputable outlets.
-
Does it use scare tactics or hype? “Doctors don’t want you to know this secret cure!” → red flag.
-
Can you fact-check it? Try NHS.uk, Full Fact (UK), Snopes, Reuters Fact Check or BBC Verify.
-
Check dates and pictures — old or unrelated content is often recycled to look new.
🚦 The traffic-light test
-
🟢 Green – from official sources, confirmed, calm tone → likely true.
-
🟡 Amber – source unclear, dramatic style, no confirmation elsewhere → pause, check.
-
🔴 Red – sensational, “miracle” claims, conspiracy, or urging you to share → almost certainly false.
💡 Should we avoid social media completely?
Not necessarily. Social media has real value for support, awareness, and connection. The key is using it wisely:
-
Follow trusted organisations for health and news.
-
Unfollow or mute accounts that regularly spread falsehoods.
-
Balance social media with direct trusted sources (NHS, GP, recognised news).
-
Step away if scrolling leaves you anxious, angry, or confused.
✨ Bottom line
False stories spread online because the system rewards attention, not accuracy. Laws and technology help, but they can’t stop misinformation entirely.
The best defence is awareness. Before acting on or sharing any post — whether about health, politics, or world events — pause, check, and if in doubt, don’t share.
👉 Protecting yourself from misinformation means protecting your community too.

When Caring for a Loved One Becomes Overwhelming: A Guide for Family Carers
Caring for a spouse, parent, or child is one of the most loving things you can do — but it can also be one of the hardest. Many family carers feel torn: wanting to give the very best care, yet struggling with exhaustion, isolation, and the feeling that “no one else can do it as well as me.”
This guide brings together insights to help you recognise when caring is becoming too heavy, why it feels so difficult to let go, and how to build a sustainable balance that protects both you and the person you love.
Why caring feels so demanding with family
-
Loss of independence: Illness often leaves people feeling powerless. Demanding behaviour can be a way of trying to regain control.
-
Role reversal stress: When a child becomes a parent’s carer, or a spouse becomes more like a nurse, both sides can feel uncomfortable.
-
Emotional safety: Patients often hold back with professionals but show raw feelings at home. That can come across as extra demanding.
-
Blurred boundaries: With family, it’s harder to say “no.” A patient may expect more than they ever would from an outsider.
When the caring role becomes unreasonable
Caring is no longer sustainable when:
-
Your health breaks down from exhaustion or stress.
-
You are completely isolated, with no time for friends, rest, or hobbies.
-
The caree’s demands exceed real need, and everything revolves around them.
-
Boundaries disappear and you can’t say no without conflict.
-
You are the only source of support, with no outside help.
These are warning signs that it’s time to rebalance the situation.
Why it doesn’t mean “defeat”
Asking for help can feel like admitting failure — but it isn’t.
-
Caring is a marathon, not a sprint. Protecting your health means you can keep caring longer.
-
Strength means knowing your limits. Bringing in help shows foresight, not weakness.
-
Love isn’t replaced. Professional carers can take tasks off your hands, but your relationship and bond remain uniquely yours.
Think of it not as “stepping back” but as building a care team. You remain the anchor, but you don’t carry everything alone.
Why it’s hard to let others help
Many carers say: “They don’t do it as well as I do.” This is natural — you know your loved one’s habits and needs better than anyone. Professionals may work differently, and that can feel uncomfortable.
But:
-
Different doesn’t always mean worse — just not “your way.”
-
Perfection isn’t sustainable if it destroys your health.
-
Your role as spouse/child/friend is irreplaceable — letting others handle routine care may free you to keep that role.
Start small: allow someone else to take over one task or cover for a short period. Gradually, trust can build.
Can problems be predicted?
Yes — carers often see the signs early:
-
Constant exhaustion or resentment
-
Dropping their own health needs or appointments
-
Losing touch with friends and community
-
Feeling guilty if they take any time for themselves
If these signs appear, it’s time to bring in extra support before crisis strikes.
Practical steps to make caring sustainable
-
Have early, honest conversations about what you can and cannot do.
-
Ask for a Carer’s Assessment (in the UK) — this can open up respite care, day services, and financial support.
-
Bring in professional support early so it feels like teamwork, not abandonment.
-
Protect your own time — even short, regular breaks keep you healthier.
-
Seek peer support — carers’ groups and counselling reduce isolation.
Final thought
Caring is an act of deep love. But love alone cannot carry the whole weight forever. Sharing the load is not defeat — it is the wisest way to ensure that both you and your loved one remain safe, cared for, and connected.
You are not failing. You are leading a team, protecting your own well-being, and preserving the relationship that matters most.
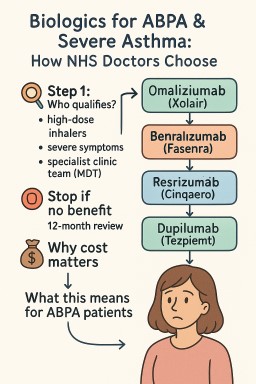
💊 Biologics for ABPA & Severe Asthma: How NHS Doctors Choose
Biologics are modern injection or infusion treatments that target the immune system. They can help people with Allergic Bronchopulmonary Aspergillosis (ABPA) by reducing inflammation, cutting down on steroid use, and lowering flare-ups.
In the UK, consultants must follow NICE (National Institute for Health and Care Excellence) guidance, which sets both clinical criteria and cost-effectiveness rules.
🔎 Step 1: Who qualifies?
-
You must already be on high-dose inhalers and still have severe symptoms.
-
Decisions are made by a specialist severe asthma / ABPA clinic team (MDT).
-
Blood tests, flare history, and steroid use are all considered.
🧭 Step 2: Which biologic?
Consultants match the drug to the type of inflammation you have:
| Pathway / Clues | Possible Biologic | Notes |
|---|---|---|
| IgE-allergic (allergic tests positive, high IgE) | Omalizumab (Xolair) | Works best if perennial allergies are driving symptoms. |
| Eosinophilic (high eosinophil counts, frequent flare-ups, or long-term steroid use) | Mepolizumab (Nucala) or Benralizumab (Fasenra) | NHS requires doctors to choose the least-expensive if both fit. |
| Eosinophils ≥400 + frequent flare-ups | Reslizumab (Cinqaero, IV drip) | Less used, but an option if IV therapy is acceptable. |
| Still severe after above / not eligible | Dupilumab (Dupixent) | Also helps if you have eczema or nasal polyps. |
| Any type, severe with ≥3 flare-ups or on daily steroids | Tezepelumab (Tezspire) | Works even if blood tests don’t show high eosinophils or IgE. |
🛑 Step 3: Stop if no benefit
NICE requires a 12-month review.
-
If your flare-ups or daily steroid dose haven’t fallen enough (usually by ≥50%), treatment should stop.
💷 Why cost matters
-
The NHS only funds biologics judged “cost-effective.”
-
If two drugs are equally suitable, consultants must use the least-expensive one.
-
This doesn’t mean you won’t get the right drug — but sometimes doctors must justify why one biologic is better for you personally.
📌 What this means for ABPA patients
-
ABPA is not directly covered by NICE guidance, but the same biologics are often used if you also meet asthma criteria.
-
Main goals:
-
Reduce oral steroids (prednisolone) and their side-effects.
-
Control flare-ups and lung damage.
-
-
Evidence supports omalizumab, mepolizumab, benralizumab, and dupilumab in ABPA; tezepelumab has less data so far.
✅ Bottom line:
Biologics can be life-changing for ABPA patients, but the NHS pathway means the choice depends on your blood results, flare history, steroid needs — and cost-efficiency rules. If one option doesn’t work, another may still be possible.
📚 New Children’s Book Helps Families Understand Aspergillosis
Launch Event at Affinity Outlet, Fleetwood – 13th September 2025
The Aspergillosis Trust is delighted to announce the launch of a brand-new children’s book, Dad and the Sneaky Spores, written by award-winning author Christina Gabbitas and beautifully illustrated by Ursula Hurst.
This story has been specially commissioned to raise awareness of aspergillosis, a serious lung condition caused by the Aspergillus fungus. Through gentle storytelling and colourful illustrations, the book helps children and families understand what it means to live with a parent affected by aspergillosis.
✨ About the Event
📅 Date: Saturday 13th September 2025
📍 Location: Affinity Outlet, Fleetwood
The launch event will be a fun and informative day for all the family.
-
✍️ Meet the Author: Christina Gabbitas will be signing copies of the book between 12pm and 2pm.
-
👩⚕️ Ask the Experts: A qualified nurse will be available to answer medical questions or offer advice.
-
📚 Learn Together: Families can explore how storytelling can make complex health conditions easier to understand.
📖 About Dad and the Sneaky Spores
The book follows a family’s journey with aspergillosis in a way that children can relate to. It not only explains the illness but also encourages empathy, resilience, and understanding within families.
“The narrative not only educates readers about aspergillosis but is also thoughtfully crafted to foster empathy and understanding.” – Aspergillosis Trust
Published by Poems & Pictures, Dad and the Sneaky Spores is available from 1st August 2025.
💜 Why This Matters
Aspergillosis is a rare and often misunderstood condition. By raising awareness through creative storytelling, this initiative provides a new way to start important conversations with children, families, and the wider community.
🔗 Find out more at: www.aspergillosistrust.org