
🤐 Why It's Important Not to Share Your Clinical Trial Experience — Until It’s Over
If you have chronic pulmonary aspergillosis (CPA), you may be invited to take part in a clinical trial for a new antifungal medication like rezafungin. That’s exciting — and could help improve treatment for many people in future.
Naturally, people want to support each other by sharing experiences, especially in online support groups. But when it comes to clinical trials, there’s a really important reason why we shouldn’t talk about how we’re feeling while we’re still in the trial.
Here’s why.
🧪 What Are Clinical Trials For?
Clinical trials help doctors and researchers answer important questions like:
-
Does this new treatment work?
-
Is it better than the current treatment?
-
What side effects might it cause?
To get accurate answers, the trial needs to be fair and unbiased — meaning that personal expectations and outside influences shouldn’t affect how people report their symptoms or progress.
📣 The Problem With Sharing During a Trial
If you’re taking part in a trial and say something like:
“I feel great — this new drug is working for me!”
or
“This is making me feel worse than ever — don’t join!”
...other people may change how they think and feel based on your comment.
This is called bias. It can:
-
Make others expect the same good (or bad) result
-
Affect how people rate their own symptoms
-
Cause people to drop out or not join at all
-
Make the trial results less accurate or even unusable
Even well-meaning comments can damage the study, especially if the trial is small (like most CPA studies are).
🕵️♀️ What If It’s a Blinded Trial?
Some trials are "blinded", meaning you don’t know whether you're getting the new treatment or a standard one (or placebo).
But if people start guessing or posting:
“I’m sure I’m on the real drug — I feel amazing!”
...then other people might also guess, or feel disappointed — which again, affects how results are reported.
🚦When Is It Safe to Share?
💬 After the trial is over and the results are published, you can talk freely about your experience.
In fact, patient voices are vital at that stage — they help others understand what it’s like to be part of a trial and whether new treatments are helpful in real life.
💡 What You Can Say During the Trial
You can still help raise awareness without compromising the study. For example:
-
✅ “I’m taking part in a CPA trial – ask your doctor if you might be eligible.”
-
✅ “There’s a study on a new antifungal — here’s the link to the official trial page: clinicaltrials.gov/study/NCT06794554”
-
✅ “I’m proud to be contributing to research — happy to share my experience once the trial ends.”
Just don’t talk about how the treatment is affecting you until the trial is complete.
🙏 Why This Matters
By keeping quiet during the trial, you're:
-
Protecting the integrity of the study
-
Helping future patients get trustworthy answers
-
Supporting the research team who need clear, unbiased data
You’re not just taking part in a trial — you’re helping build evidence that others will depend on for years to come.
🧭 Summary
| ✅ Do | ❌ Don’t |
|---|---|
| Tell people a trial exists | Share how the treatment is affecting you |
| Encourage others to talk to their doctor | Post guesses about which drug you’re on |
| Wait until the trial ends to share experiences | Influence others to join based on your results |
If you're ever unsure, ask your clinical trial team or group moderator — they'll be glad to help. Your role in research is important, and your silence now is a powerful act of support for science, fairness, and future care.

🧾 Rezafungin: A New Antifungal Being Trialled for CPA
Some people with chronic pulmonary aspergillosis (CPA) have trouble tolerating standard antifungal medications. Commonly used drugs like voriconazole and posaconazole can cause serious side effects such as hallucinations, liver enzyme disturbances, or gut problems. When these medications can’t be used, options become limited.
A new antifungal, rezafungin, is now being studied as a possible treatment for CPA — especially in people who can't tolerate azoles. It is not yet approved for aspergillosis, but a major clinical trial is under way.
🧬 What Is Rezafungin?
Rezafungin is part of a newer group of antifungal drugs called echinocandins. These work by weakening the fungal cell wall — a very different mechanism to azole drugs like itraconazole or voriconazole.
Key features:
-
Given as a weekly intravenous (IV) drip
-
Long-acting: stays in the body for days after each dose
-
Designed to provide high drug levels in the lungs and bloodstream
-
Early studies show less frequent side effects than with some older antifungals
It is already licensed for treatment of Candida bloodstream infections but is being studied now for CPA.
🧪 Current Research: Trial for CPA
A clinical trial is currently recruiting people with CPA who:
-
Cannot take azole antifungals because of side effects or resistance
-
Need alternative or combination therapy
This trial (called REZAFUNGin Efficacy and Safety for Aspergillus – CPA) is being conducted in the UK and internationally. The goal is to test whether rezafungin is safe and effective in CPA patients who have few remaining options.
🔗 View the clinical trial (NCT06794554)
📊 What Have Previous Studies Found?
While studies in CPA are just beginning, previous trials in other fungal infections provide important clues:
✅ Phase 2 & 3 Studies (Candida Infections)
-
Rezafungin was found to be as effective as daily echinocandins (like caspofungin)
-
Once-weekly dosing worked just as well as daily treatment
-
Side effects were mild, and liver toxicity was rare
-
No CNS side effects (like hallucinations) were reported
🧫 Laboratory Evidence
-
Rezafungin is active against Aspergillus fumigatus, including some azole-resistant strains
-
It reaches good levels in lung tissue — an important feature for CPA
-
May be used alone or with another antifungal in complex cases
🩺 Case Example
A recent case report described successful treatment of chronic pulmonary aspergillosis using rezafungin plus voriconazole in a patient with resistant infection (Oxford University Press, 2024).
⚠️ Is Rezafungin Available Now?
Not yet. Rezafungin is only available for CPA:
-
Through a clinical trial, or
-
By special approval for compassionate use in selected cases
It is not currently licensed for aspergillosis in the UK or elsewhere.
💬 What Should I Discuss with My Doctor?
If you're considering participation in a clinical trial or if standard treatments have failed, you might ask:
-
Am I eligible for the rezafungin CPA trial?
-
What are the benefits and risks of trying this treatment?
-
Will I still need other antifungals (e.g. azoles or amphotericin)?
-
How often will I need blood tests and hospital visits?
-
Will this help if I have azole resistance or liver side effects?
📌 Summary
Rezafungin is a new antifungal drug being tested for people with chronic pulmonary aspergillosis who cannot take older treatments. It offers once-weekly dosing and early signs suggest a favourable safety profile, including in patients with liver concerns or those who had side effects from azoles.
Although not yet widely available, it may offer hope for people with limited options. If you or someone you know is struggling with antifungal intolerance, you may wish to speak to your medical team about the CPA clinical trial or explore compassionate access routes.
👉 Learn more or check trial sites:
🔗 https://clinicaltrials.gov/study/NCT06794554
Cyber Safety for Aspergillosis Patients: Supplement to UK NCSC Advice
This guide builds on the official UK Government cybersecurity advice for families and individuals (www.ncsc.gov.uk/section/advice-guidance/you-your-family) and adds patient-specific tips for people with aspergillosis.
Feeling overwhelmed?
You're not alone. The internet and phone landscape can feel like a minefield, especially when you're trying to manage your health too. No one expects you to become an expert in cybersecurity overnight. The aim of this guide isn’t to scare you — it’s to help you take small, realistic steps to protect yourself.
Just like with your health, doing the basics well goes a long way. You don’t need to memorise everything — focus on:
- Using strong passwords (or a password manager)
- Being cautious with texts, links, and phone calls
- Asking for help when something doesn’t feel right
- Always accept updates on your phone, browser, or computer when offered — these often fix known security problems and help keep you protected.
It's okay to stop and ask: “Does this sound right?” If in doubt, check with someone you trust.
Top Scam Red Flags
Watch out for these common signs that something could be a scam:
- You’re told to act urgently or keep it secret
- You’re offered money, discounts, prizes or help out of the blue
- You’re asked to click a link or open an attachment in a message
- A caller claims to be from the bank, NHS, government, or police, but something feels off
- You’re told the second part of a message will come from a different number or address
- You’re asked to confirm personal, financial or password information
- You’re asked to download software or apps to “fix” your device
- You’re pressured to stay on the phone or not call anyone else
If in doubt, hang up, delete, or double check with someone you trust.
1. Protecting Your NHS and Medical Accounts
- Use strong, unique passwords for your NHS login, GP apps (e.g. Patient Access, myGP), or hospital portals.
- Enable two-factor authentication (2FA) wherever it’s offered.
- Never share your NHS login or codes with anyone.
- Always go directly to the official app or website, not through links in emails or texts.
2. Beware of Scams
- Scams can take many forms — phone calls, emails, texts, or fake websites.
- Be especially wary of anyone offering money, discounts, prizes, or urgent deals.
- Criminals may pose as trusted organisations like your bank, utility provider, government, or even the NHS.
- As a general principle: if something seems too good to be true — such as offers of free money, major discounts, prizes, or miracle cures — it almost certainly isn't real. Be suspicious of anything that promises unusually high benefits for little or no effort.
- If in doubt, forward suspicious messages to [email protected] (Link) or speak to someone you trust before taking action.
3. Using Online Support Groups Safely
- Facebook groups and forums can be great for connection, but don’t post:
- Your address, phone number, or full date of birth
- Photos of prescriptions or test results
- Don’t click links shared by strangers, even if they seem friendly.
- Moderators or admins should never ask for sensitive personal details.
4. Shopping and Donations
- Be cautious when buying medical supplies or donating online.
- Stick to trusted UK pharmacies and charities.
- Watch for copycat sites that look like legitimate health organisations.
5. Email, Phone & Text Safety
- Don’t click on links or open attachments in messages claiming to be from the NHS, unless you were expecting them.
- Never share passwords or bank details over email or text.
- Never give out your account numbers or passwords, especially if someone is trying to rush or pressure you.
- Scam texts can fake NHS or GOV.UK addresses — check official sites if unsure.
- Even texts or emails that appear to come from your bank can be faked. A common red flag is a message saying that a second text or email will come from a different number or sender — ask yourself why a genuine organisation would do this. Real authorities go to great lengths to be verifiable.
- If someone calls and tries to rush or scare you, hang up and call back using an official number from the NHS or your GP’s website.
- If in doubt — or even as a general principle — hang up and call a number you can verify yourself, such as:
- The number printed on the back of your bank card
- The official website of a company or authority (searched independently)
- Avoid using any contact information provided by the caller or in a suspicious message — treat it as untrustworthy until confirmed.
- To check a suspicious link in a text, don’t click — instead, search for the organisation’s website directly or ask someone you trust.
6. If You're Shielding or Vulnerable
- You may be more targeted by scams pretending to offer:
- COVID-19 test kits, antifungal treatments, or priority delivery slots
- Access to urgent medical appointments or services
- Verify any offer with your NHS care team before taking action.
7. Keeping Your Devices Safe
- Install antivirus and keep your phone/tablet/computer updated.
- Always accept software updates — they patch security flaws that criminals may try to exploit.
- Set devices to auto-lock and use a passcode or fingerprint.
- Avoid using public Wi-Fi for medical logins or financial information.
Do You Still Need Antivirus?
- Windows PCs: Yes — always install antivirus. Microsoft Defender (built-in) is good and free. You can also consider free versions of AVG, Avast, or Bitdefender.
- Mac computers: Less targeted, but still recommended. Free options include Avira or Sophos Home.
- Android phones: A good idea, especially if you install apps outside the Play Store. Try Bitdefender or AVG.
- iPhones/iPads: Antivirus apps aren’t usually needed if you keep iOS updated and install apps only from the App Store.
Whichever device you use, updates and cautious browsing are just as important as antivirus software.
8. Best Ways to Use Strong Passwords
Cyber security can be time-consuming and even irritating — but as malicious activity becomes more sophisticated, it’s worth the effort. Consider using different levels of passwords for different kinds of accounts:
- Low-level passwords for things like newsletters or forums
- High-level, strong passwords for NHS, banking, or health-related logins
Make Passwords Long and Unique
- Use at least 12 characters, mixing letters, numbers, and symbols
- Avoid personal info like names or birthdates
Use a Password Manager
- Tools like Bitwarden, 1Password, or Apple Keychain securely store passwords
- You only need to remember one master password
Use Passphrases for Important Accounts
- Combine random words to create a memorable but strong password, like:
Correct!Horse-Battery!Staple99
Turn On Two-Factor Authentication (2FA)
- Adds a second layer of protection, such as a code from your phone
- 2FA ties your account to a specific device (like your phone), meaning a criminal would need access to that device as well as your password to break in
Use a Unique Password for Every Account
- Never reuse passwords
Avoid These Mistakes
| Mistake | Better Option |
|---|---|
| Reusing passwords | Use a password manager |
| Writing them down | Use encrypted storage |
| Adding "123" to a word | Use unrelated, random words/symbols |
When to Change Passwords
- If your account may have been hacked
- If the same password is used elsewhere
Is It Safe to Use Chrome or Other Browser Autofill?
Using Chrome, Firefox, Safari, or Edge to autofill logins can be safe with the right precautions:
- Your device should be private and locked with a passcode or fingerprint
- Your browser and operating system should be kept fully up to date
- You should avoid storing logins for sensitive accounts (e.g. banking, NHS login)
Risks to consider:
- Passwords stored in browsers can be accessed by malware or rogue extensions
- If someone gets access to your device, they may access saved logins
Safer Alternative:
- Use a dedicated password manager (like Bitwarden, 1Password, or Dashlane)
- These offer stronger security and are harder for malware or hackers to access
If you do use browser autofill, protect your device and account with:
- Two-factor authentication for your Google, Apple, or Microsoft account
- A strong device password or biometric lock
9. Finding the Happy Medium
Cybersecurity doesn’t have to take over your life — the key is to find a realistic balance between staying safe and staying sane:
- Focus on protecting your most important accounts first — especially NHS, email, banking, and anything medical
- Don’t ignore warning signs, but don’t feel you have to be perfect with every app or device
- Use automation where possible (e.g. password managers, browser autofill, device lock)
- Ask for help if you’re unsure — carers, family members, or digital support charities can assist
Think of it like seatbelts — you hope you never need them, but they’re worth the hassle when something goes wrong.
Useful Links
- UK NCSC advice for individuals & families - constantly updated and UK government verified: https://www.ncsc.gov.uk/section/advice-guidance/you-your-family
- Report phishing emails: [email protected]
Remember: Your health is private and valuable. Treat your medical and personal information like you would your bank details. Stay cautious, ask questions, and when in doubt, ask a trusted health professional or carer.
🫁 Is It an ABPA Flare or a Bronchiectasis Flare? How to Tell the Difference
If you have aspergillosis, especially ABPA (Allergic Bronchopulmonary Aspergillosis) and bronchiectasis, it can be hard to know which one is flaring up when your lungs feel worse. They often overlap — but there are some clues that can help.
🔍 How the Two Conditions Are Different
| Feature | ABPA Flare (Allergic Reaction to Aspergillus) | Bronchiectasis Flare (Infection in Damaged Airways) |
|---|---|---|
| Main cause | Your immune system reacting to Aspergillus | Infection in widened, inflamed airways |
| Symptoms you may notice | - Chest tightness or wheezing - Thick, sticky mucus - Feeling more tired - Occasional low-grade fever |
- Wet cough with more sputum - Sputum changes colour (green/yellow) - Fever, chills, or general unwell feeling |
| How it starts | May come on gradually or after exposure to damp/mould | Often starts after a cold or virus |
| What helps most | Steroids (inhaled or oral), sometimes biologics | Antibiotics and chest physiotherapy |
| What tests may show | - Raised IgE or eosinophils - CT may show mucus plugs |
- Raised CRP or white cells - Sputum may grow bacteria or fungus |
| What to ask your doctor | “Is my IgE or eosinophil count up?” | “Do I need a sputum test or antibiotics?” |
🧭 What Can You Do as a Patient?
-
📝 Keep a symptom diary – especially note changes in:
-
Sputum colour or amount
-
Wheezing or chest tightness
-
Tiredness or sleep quality
-
-
🧪 Ask for the right tests:
-
Blood tests like IgE and eosinophils for ABPA
-
CRP, white blood count, and sputum tests for bronchiectasis
-
-
🩺 Don’t guess or self-treat – steroids and antibiotics work in different ways, and using the wrong one can make things worse or mask important signs.
💬 Final Thought
It's very common for people with aspergillosis to feel confused by flare-ups — you're not alone. Learning to spot your own patterns, and getting support from your specialist team, can make a real difference.
Asthma & Lung: 5 tips to help you breathe better and stay well
Dr Andy offers five tips to help you breathe better and stay well.
We know that things like hay fever, air pollution and hot weather can make breathing more difficult and stop you doing the things you love. Our clinical lead, Dr Andy, offers five tips to help you breathe better and stay well. Head to our website to find more easy-to-follow tips and advice to improve your breathing during the warmer months: https://orlo.uk/v9JT2
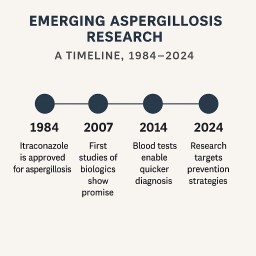
🔬 Emerging Research for Aspergillosis
Aspergillosis is a complex group of diseases caused by the Aspergillus fungus. Ongoing research is uncovering new ways to diagnose, treat, and prevent these conditions—offering hope for improved care and long-term outcomes. This page outlines current areas of promising research relevant to patients, carers, and healthcare professionals.
⏱️ Has Research Accelerated Over Time?
Yes. Over the last 40 years, research into aspergillosis and fungal infections has significantly accelerated due to:
- Rising awareness of fungal diseases in immunocompromised patients
- Improved diagnostic technology (e.g. PCR, lateral flow tests, next-gen sequencing)
- New drug development in response to growing azole resistance
- Greater investment from both academic institutions and industry
- Dedicated centres like the UK National Aspergillosis Centre driving specialist research
- Fungal infections gaining WHO recognition as emerging public health threats
In the 1980s and 1990s, progress was relatively slow. Since the early 2000s—and especially after the COVID-19 pandemic revealed the risks of fungal co-infection—momentum has increased markedly.
1. 🧪 Antifungal Drug Development
Resistance to azole antifungals is a growing concern. Several new antifungal agents are in development:
🔸 Olorofim (F2G)
- First-in-class orotomide antifungal
- Shows activity against Aspergillus, including azole-resistant strains
- Currently in phase III trials for invasive and chronic pulmonary aspergillosis
🔸 Ibrexafungerp and Fosmanogepix
- New antifungals with different mechanisms of action
- Potentially effective in combination or for resistant cases
🔸 Inhaled Antifungals
- Trials of inhaled itraconazole, posaconazole, and PC945 (opelconazole) for direct delivery to the lungs
- Aim: higher local drug concentrations with fewer side effects
2. 🧬 Biologics and Immune Modulation
🧭 What's Next in Biologic Therapies for Severe Asthma?
Several next-generation biologics are under development, aiming to:
- Broaden coverage for patients who don't respond to existing biologics
- Target upstream pathways (beyond IL‑5, IL‑4/13, or IgE)
- Offer once-yearly dosing or dual-target activity
Examples include:
- Depemokimab: A long-acting anti-IL‑5 antibody in phase 3 trials (GSK)
- CSJ117: An inhaled anti-TSLP monoclonal antibody fragment (Novartis)
- RG6354: Targeting IL-33 pathway, an upstream trigger in type 2 and non-type 2 asthma
- Dual Biologics: Exploratory research combining two targets (e.g., IL‑5 + IL‑4 or TSLP + IL‑13)
These developments may also benefit subsets of aspergillosis patients with severe asthma or ABPA who have not fully responded to current biologics. Research is exploring biologic therapies that reduce allergic inflammation or modulate immune response, particularly for ABPA (Allergic Bronchopulmonary Aspergillosis) and overlapping asthma subtypes.
✅ Biologics Currently in Use for ABPA
Omalizumab (Xolair) – Anti-IgE
- Target: IgE antibody—blocks allergic immune response to Aspergillus antigens.
- Evidence: Studies show significant reductions in exacerbations, IgE, steroid use, and improved lung function.
- Clinical Use: Widely used off-label in ABPA patients with raised IgE and asthma features.
Mepolizumab (Nucala) – Anti–IL‑5
- Target: IL‑5 cytokine—reduces eosinophil inflammation.
- Use: Steroid-sparing and symptom control in eosinophilic ABPA.
Benralizumab (Fasenra) – Anti–IL‑5 Receptor
- Target: IL‑5Rα—causes rapid eosinophil depletion.
- Use: Clearing mucus plugs and reducing flares; often used after mepolizumab failure.
Dupilumab (Dupixent) – Anti–IL‑4Ra
- Target: IL‑4/IL‑13 pathway—type 2 inflammation.
- Use: Shown to reduce IgE levels and ABPA exacerbations.
Tezepelumab (Tezspire) – Anti‑TSLP
- Target: TSLP—broadly suppresses upstream allergic inflammation.
- Evidence: Early reports suggest benefit in ABPA patients, though data are limited.
📊 Real-World Effectiveness
UK-based retrospective study (2014–2022):
- 74 ABPA patients treated with biologics
- 65% showed ≥50% reduction in steroid use after 12 months
- 35% switched due to lack of effect or side effects
📌 Summary Table of Biologics
| Biologic | Target | Use in Aspergillosis | Key Benefits |
|---|---|---|---|
| Omalizumab | IgE | ABPA with raised IgE | ↓ Exacerbations, ↓ steroids, ↑ FEV₁ |
| Mepolizumab | IL‑5 | Eosinophilic ABPA | Steroid-sparing, symptom control |
| Benralizumab | IL‑5Rα | Refractory cases | Mucus clearance, eosinophil depletion |
| Dupilumab | IL‑4/IL‑13 | Mixed allergic/eosinophilic ABPA | ↓ IgE, ↓ flares |
| Tezepelumab | TSLP | Emerging, broad asthma-ABPA | Broad inflammation control |
3. 🧫 Diagnostic Advances
Improved diagnostics aim to detect disease earlier and more accurately:
- Lateral flow tests (e.g., Aspergillus-specific LFD) for rapid diagnosis
- PCR testing and galactomannan assays in blood, sputum, or BAL
- Aspergillus-specific IgG and IgE testing to distinguish CPA, ABPA, and colonisation
- Next-generation sequencing (NGS) for strain typing and resistance detection
4. 🌡️ Non-Pharmacological Research
🌀 Airway Clearance and Physiotherapy
- Trials assessing flutter devices, oscillating PEP, and manual physiotherapy in chronic aspergillosis and bronchiectasis
🥦 Nutrition and Gut-Lung Health
- Increasing interest in the role of dietary fibre, gut microbiome, and short-chain fatty acids in immune defence and lung inflammation
💨 Air Quality and Exposure
- Home-based studies evaluating the impact of HEPA filters, spore counts, and environmental remediation
5. 🛡️ Preventative Strategies
🫁 Lung/Nasal Coatings (Experimental)
- Early research into coating the lungs or nasal passages to prevent infection
- Not yet in human trials for aspergillosis, but promising in animals for viral and bacterial prevention
💉 Vaccines
- No approved vaccines yet, but exploratory work is underway for high-risk populations
6. 🧫 Clinical Trials in Aspergillosis
A wide range of clinical trials are currently underway or recently completed, focusing on new antifungals, biologics, and non-pharmacological interventions:
🧪 Antifungal Trials
- Rezafungin – A long-acting echinocandin administered once weekly, currently in trials for prevention and treatment of invasive fungal infections, including those caused by Aspergillus species
- Olorofim (F2G) – Phase III trials for CPA and invasive aspergillosis
- PC945 (Opelconazole) – Inhaled triazole for CPA and prophylaxis in immunocompromised patients
- Fosmanogepix and Ibrexafungerp – Investigated in resistant and invasive fungal disease
🧬 Biologic Trials
- Tezepelumab and Dupilumab – Trials involving patients with ABPA and severe asthma
- Depemokimab (GSK) – Phase III trials for long-acting IL‑5 blockade
🌡️ Other Trials
- Airway clearance studies – Use of physiotherapy and flutter/PEP devices in chronic pulmonary aspergillosis
- Gut microbiome and fibre supplementation – Exploring anti-inflammatory potential in lung disease
These trials often recruit patients from UK centres including the National Aspergillosis Centre, and are registered on databases such as ClinicalTrials.gov.
7. 🤝 Patient Support and Outcomes Research
📊 Real-World Evidence
- Registries and observational studies (e.g., LIFE, FungiScope) gathering long-term data on patients with CPA, ABPA, SAFS, and invasive disease
👥 Quality of Life and Patient-Reported Outcomes
- Surveys and tools to measure impact of fatigue, breathlessness, mental health, and medication side effects
- Aim: improve personalised care and support services
🧭 Where to Find Updates
- ClinicalTrials.gov – searchable by "aspergillosis"
- Aspergillosis.org – for patient-friendly research summaries
- National Aspergillosis Centre (UK) – involved in many UK-based studies
- Journal of Fungi, Medical Mycology, Clinical Infectious Diseases – leading sources of peer-reviewed studies
📢 Final Word
Research into aspergillosis is accelerating across drug development, diagnostics, prevention, and patient support. While not all options are available yet, many are in trials or early clinical use. Staying informed and involved—whether through trial participation or feedback—helps shape better care for all.
Updated July 2025 – suitable for patients, clinicians, and advocacy groups.
🫁 Could Lung or Nasal Coatings Help Prevent Aspergillosis?
As research into new ways of preventing lung infections advances, some patients with aspergillosis are asking whether coating the lungs or airways—with a protective spray, gel, or surfactant—might one day protect them from fungal disease.
Here’s what the science says so far.
🔬 What Is Being Researched?
Scientists are currently studying ways to coat the lungs or nasal passages with a protective substance designed to:
- Trap or neutralise viruses, bacteria, or fungal spores
- Stabilise the lung or airway lining
- Prevent inflammation or infection from taking hold
These coatings may come in the form of:
- Dry powder aerosols (inhaled)
- Drug-free nasal gels or sprays
Importantly, these are being developed as preventative measures, not as treatments for people already ill.
🧪 Current Research: Early-Stage, Not Yet for Aspergillosis
1. Dry Powder Lung Surfactants
- These are based on natural surfactants that coat the lungs and keep the air sacs (alveoli) open.
- Tested in animals (e.g., lambs, rabbits) with good results in preventing respiratory distress or injury.
- Used mostly in neonatal care for premature babies.
- Not yet tested for fungal infections or chronic diseases like aspergillosis.
2. Nasal Gel-Coating Sprays
- These sprays form a temporary coating in the nose and upper airways, shown in mice to block viruses like flu or COVID-19.
- Protective effect may last several hours.
- Still in animal testing—no human trials or approvals yet.
- No evidence yet that they can prevent fungal infections like Aspergillus.
📌 Are These Coatings Available Yet?
No. As of now:
- There are no licensed lung or nasal sprays designed to prevent aspergillosis or other fungal lung infections.
- Most studies are in pre-clinical stages (animal research only).
- It may be several years before any human trials begin.
🛡️ Who Might Receive These Preventatives in the Future?
If future research proves these coatings are safe and effective, likely priority groups would include:
🎯 High-risk populations:
- People with chronic aspergillosis (CPA) or ABPA
- Patients on long-term steroids or immunosuppressants
- Individuals with bronchiectasis, COPD, or cystic fibrosis
- Transplant recipients or those with cancer or immune deficiencies
- Elderly people, especially in care homes
- Healthcare or construction workers exposed to dust, spores, or mould
- Hospitalised or ventilated patients (e.g. risk of CAPA in ICU)
❗ What Aspergillosis Patients Should Know
- These technologies are not available yet and remain in the research phase.
- They are being explored as preventative tools, not as treatment for existing fungal infections.
- There is no evidence yet they can prevent Aspergillus infections—but the research is promising.
✅ What You Can Do Now
Until better preventatives are developed, people with aspergillosis can reduce risk by:
- Avoiding high-risk environments (e.g., compost, renovation dust, decaying vegetation)
- Using prescribed antifungals or steroids correctly
- Supporting immune health (e.g., good nutrition, rest, fibre-rich diet)
- Asking doctors about biologics or ongoing research trials if relevant
📘 Final Word
While the idea of coating the lungs or nose to stop infections sounds futuristic, it’s grounded in real science. For people vulnerable to fungal lung disease, this kind of innovation may one day offer protection—especially for those on immunosuppressive treatments or with fragile lungs.
But for now, the best defence remains personalised treatment, avoidance strategies, and good communication between specialists and GPs. We’ll keep watching this space closely as research develops.

🌾 Dietary Fibre and Disease Prevention: Why We Need to Eat More Fibre
Fibre is no longer just about bowel regularity. Modern research shows that dietary fibre plays a fundamental role in overall health, immune regulation, and chronic disease prevention. Low-fibre diets are now being linked to a growing list of physical and mental health conditions, with multiple sclerosis (MS) among the most recent examples.
🔍 What Is Dietary Fibre?
Fibre is the indigestible part of plant-based foods that helps regulate digestion, supports beneficial gut bacteria, and contributes to metabolic and immune function. The two main types are:
- Soluble fibre: dissolves in water, forms a gel-like substance, and helps control blood sugar and cholesterol
- Insoluble fibre: adds bulk to stool and supports bowel regularity
🚨 How Much Fibre Do We Need?
- UK recommendation: 25–30g/day for adults
- Average intake: only around 18g/day
- This means most people are getting 25–40% less fibre than they need
🩺 Diseases Linked to Low Fibre Intake
A growing body of evidence links low-fibre diets to:
Digestive & Gastrointestinal Disorders
- Constipation
- Diverticular disease
- Haemorrhoids
- Irritable bowel syndrome (IBS)
Metabolic and Cardiovascular Diseases
- Type 2 diabetes (via insulin resistance and glucose spikes)
- Obesity (through reduced satiety and changes to the microbiome)
- High cholesterol
- Cardiovascular disease
Cancer
- Colorectal cancer risk is significantly reduced by high-fibre diets (especially cereal fibre)
Inflammatory & Autoimmune Conditions
- Multiple sclerosis (MS): recent research links gut microbial imbalance, worsened by low fibre, to inflammation and autoimmunity
- Inflammatory bowel disease (IBD): fibre can help regulate gut inflammation in some forms
- Rheumatoid arthritis and asthma: animal studies suggest protective roles
Brain and Mental Health
- Anxiety and depression: linked to gut-brain axis disruption when fibre is insufficient
- Neuroinflammation: fibre supports short-chain fatty acid production (e.g. butyrate), which helps reduce inflammation that affects brain and mood
🧬 Why Fibre Matters for the Gut Microbiome
Fibre is the main energy source for beneficial gut bacteria. These microbes ferment fibre into:
- Short-chain fatty acids (SCFAs) like butyrate, propionate, and acetate
- These SCFAs:
- Nourish the gut lining
- Modulate immune responses
- Reduce systemic inflammation
- Influence brain function via the gut–brain axis
Low fibre leads to:
- Less microbial diversity
- More pro-inflammatory bacteria
- Greater permeability of the gut wall ("leaky gut")
🥦 How to Increase Fibre Intake
🥣 Everyday Fibre-Rich Food Ideas
Here are some simple, everyday options to help boost your fibre intake, with estimated fibre content:
| Food Item | Approximate Fibre (g) per Serving |
|---|---|
| Muesli (40g serving with fruit & seeds) | 6–8g |
| Porridge oats (40g) | 4g |
| Wholemeal toast (2 slices) | 5–6g |
| Nut butter (1 tbsp) | 1–2g |
| Lentil or bean soup (1 bowl) | 7–10g |
| Chickpeas in salad (half cup) | 6g |
| Brown rice (1 cup cooked) | 3–4g |
| Quinoa (1 cup cooked) | 5g |
| Berries (1 cup) | 4–8g (depending on type) |
| Apple or pear (with skin) | 3–4g |
| Banana (medium) | 3g |
| Nuts or seeds (30g handful) | 2–4g |
| Air-popped popcorn (3 cups) | 3–4g |
🚫 Common Low-Fibre Foods
Many widely consumed foods contain very little or no dietary fibre, especially if they are highly processed or refined. Examples include:
| Food Item | Approximate Fibre (g) |
| White bread (2 slices) | 1g or less |
| White rice (1 cup cooked) | 0.5–1g |
| White pasta (1 cup cooked) | 1–2g |
| Processed breakfast cereals | 1–2g |
| Biscuits and cakes | <1g per portion |
| Ready meals (typical portion) | 1–2g |
| Crisps / potato chips (25g) | <1g |
| Soft drinks, fruit juice (250ml) | 0g |
| Cheese, meat, and eggs | 0g |
These low-fibre foods dominate many modern diets. Without mindful inclusion of whole plant foods, it is easy to fall well below the recommended fibre intake.
💡 Is It Easy to Reach the Target? These can be rotated across meals and snacks to easily reach your fibre goals without drastic changes.
⚖️ What If Fibre Causes Looser Bowels?
It's not uncommon for people to experience looser stools, more frequent bowel movements, or mild bloating when increasing fibre intake too quickly. This usually happens because:
- The gut bacteria are adjusting to more fermentable material
- Insoluble fibre speeds up gut transit time
The good news:
- These effects are usually temporary and settle within a few days to a couple of weeks
- You can achieve a happy medium by:
- Increasing fibre gradually over 1–2 weeks
- Including both soluble (e.g. oats, pulses, fruit) and insoluble (e.g. wholemeal bread, bran) fibre
- Drinking plenty of water
If symptoms continue, consult a GP or dietitian—especially if you have conditions like IBS or IBD that affect gut sensitivity.
✅ Summary
| Area of Health | Fibre Benefits |
| Gut & digestion | Regularity, reduced IBS/diverticulitis |
| Heart & metabolism | Lower cholesterol, improved glucose control, satiety |
| Immune system | Less inflammation, gut barrier protection |
| Mental health | Gut–brain axis modulation, reduced neuroinflammation |
| Cancer prevention | Lower colorectal cancer risk |
🌿 Special Note for People with Aspergillosis
If you are living with aspergillosis, especially chronic forms like CPA or ABPA, or regularly take medications such as antifungals, corticosteroids, or antibiotics, fibre is particularly important:
- Antibiotics can disrupt gut microbiota, reducing beneficial bacteria and fibre fermentation
- Steroids can impair immune regulation and blood sugar control, both of which benefit from high-fibre diets
- Antifungals and long-term illness may alter digestion or appetite, making a high-quality, fibre-rich diet even more essential
Maintaining a healthy gut environment through a fibre-rich diet may help support immunity, reduce inflammation, and improve resilience to infection and medication side effects.
📢 Final Note
Fibre is now a front-line defence against modern disease. It's one of the most underconsumed but powerful nutrients for preventing chronic illness, improving resilience, and nurturing a healthy gut microbiome.
Recent links to conditions like multiple sclerosis highlight just how far-reaching fibre’s impact may be—making it more than a digestive aid, but a foundation of systemic health.

💙 Disability Verification and Support for People with Aspergillosis in the UK
Living with aspergillosis—whether it's chronic pulmonary aspergillosis (CPA), allergic bronchopulmonary aspergillosis (ABPA), or another form—can have a significant impact on daily life. Many people find that fatigue, breathlessness, medication side effects, and other long-term symptoms affect their ability to work, care for themselves, or maintain independence.
If your condition is affecting your daily activities, you may be entitled to disability support, financial help, or adjustments at work or home. This guide explains how to get your disability recognised and verified in the UK, who can help, and how this varies across age groups and types of disability.
✅ What Counts as a Disability?
Under the Equality Act 2010, a person is classed as disabled if they have:
“A physical or mental impairment that has a substantial and long-term negative effect on their ability to carry out normal day-to-day activities.”
Many people with aspergillosis meet this definition—especially if they experience breathlessness, fatigue, pain, or recurrent infections over months or years.
📋 How Can You Prove or Verify Your Disability?
There is no single "disability certificate" in the UK. Instead, different systems accept different types of evidence, depending on what support you are applying for.
1. Benefit Award Letters
These are the most commonly accepted form of disability evidence:
- Personal Independence Payment (PIP)
- Disability Living Allowance (DLA) (for under 16s)
- Attendance Allowance (for over State Pension age)
- Employment and Support Allowance (ESA) (Support Group)
- Industrial Injuries Disablement Benefit
Where to get it: Contact the DWP or check your online account for a copy of your award letter.
2. NHS Medical Letters
Ask your GP or consultant to write a letter that:
- Confirms your diagnosis (e.g. CPA, ABPA)
- Describes the symptoms and how they affect your daily life
- Explains any treatments you need (e.g. antifungals, oxygen, steroids)
- States any long-term prognosis or care needs
3. Blue Badge and Disabled Bus Pass
- Blue Badge: Available from your local council for parking needs
- Disabled Bus Pass: Also issued locally; often requires proof of benefits or medical need
4. Occupational Therapy Assessment
- NHS or council-based OTs can assess your ability to manage daily tasks and recommend adaptations or support.
- Access via GP or Adult Social Care team.
5. Workplace or Education Support
- Occupational Health assessments may recommend reasonable adjustments such as flexible hours, remote work, or cleaner air environments.
- You may be eligible for Access to Work grants.
6. PIP and Other Benefit Assessments
- Assessments focus on how your condition affects daily tasks like mobility, personal care, medication management, and communication.
🔢 Do We Get a Disability Percentage?
In the UK, disability is not usually measured as a percentage. Most systems use functional assessments or point-based scoring.
The Exception: Industrial Injuries Disablement Benefit (IIDB)
- Uses a percentage system based on the extent of permanent disablement from a work-related condition.
For Everyone Else:
- PIP, DLA, and ESA use points-based systems.
- Employers, schools, and councils assess need based on impact, not percentage.
🡥 Who Can Help You with Disability Assessment?
| Professional / Service | Role & When to Use |
|---|---|
| GP or Specialist Consultant | Confirm diagnosis and functional impact for letters and forms |
| Occupational Therapist (NHS) | Assess your ability to manage daily tasks, recommend home aids/adaptations |
| Occupational Health (Work) | Recommend workplace adjustments under Equality Act |
| Adult Social Care (Council) | Assess for care support and home adaptation funding |
| Citizens Advice / Disability Charities | Help with forms, appeals, and understanding your rights |
| National Aspergillosis Centre (NAC) | May provide supporting letters for housing or benefits if you're under their care |
👶 Children and Young People
Under 16
- Claim Disability Living Allowance (DLA)
- Apply for an Education, Health and Care Plan (EHCP) if they have learning or developmental needs
- Get support from social care and school SENCOs
Age 16–25
- Transition to PIP for disability benefits
- EHCP can continue to age 25 if still in education
- Access workplace/education adjustments and Access to Work
- Shift from Children’s Services to Adult Social Care at 18
👵 Older Adults (Typically Age 65+)
Attendance Allowance
- For care needs only (not mobility)
- Not means-tested
Care and Support Needs
- Request a Care Act assessment from local council
- May result in home care, adaptations, or care home funding
NHS Continuing Healthcare
- For those with severe, complex needs
- Fully funded by NHS; not means-tested
Blue Badge Scheme
- Still accessible based on breathlessness or mobility limitation
Carer Support
- Carer's Assessment available
- Access to Carer’s Allowance or respite care
🧠 Mental Illness and Long-Term Invisible Disabilities
Mental health conditions and other non-visible disabilities (e.g. chronic fatigue, fibromyalgia, autism, long COVID) are also recognised under the Equality Act if they are long-term and impact daily life.
Differences in Assessment
- Focus is on non-physical activities:
- Planning and following journeys
- Managing therapy or medication
- Social interaction
- Decision-making
Key Evidence
- GP letters
- Psychiatrist or psychologist reports
- Occupational therapy or carer evidence
Support Services
- Community mental health teams (CMHT)
- Crisis teams, counselling, and talking therapies
- Supported housing or assisted living
Reasonable Adjustments
- Flexible schedules, quiet spaces, remote work
- Mental health support plans at school, university, or work
Advocacy
- Mind, Rethink, Disability Rights UK, and VoiceAbility provide advocacy, appeals help, and representation
📚 Summary Table
| Area | Physical Disabilities | Mental Health / Invisible Disability | Children | Older Adults |
| Benefit | PIP / ESA | PIP / ESA | DLA | Attendance Allowance |
| Social Care | Adult Social Care assessment | Adult Social Care or MH services | Children’s Services | Adult Social Care |
| Education/Work Support | Access to Work, OH reports | Access to Work, reasonable adjustments | EHCP, SENCO | Retirement/flexible options |
| Blue Badge | Based on mobility | Based on anxiety/severe distress for travel | May be available | Common for respiratory limits |
| Evidence Needed | Consultant, OT, GP | Psychiatrist, GP, carer, advocate | School or paediatric reports | GP, consultant, OT |
| Advocacy Support | Citizens Advice, Scope | Mind, Rethink, Disability Rights UK | IPSEA, Contact | Age UK, Carers UK |
🙏 Final Tips
- Keep copies of all letters, forms, and award notices.
- If your condition fluctuates, keep a symptom diary to show variable impact.
- Apply for assessments early as processes can take time.
- If you need help applying, speak to Citizens Advice or a local disability advocacy service.
- The National Aspergillosis Centre may be able to support patients with evidence for housing, benefit, or support applications.
🤔 Is It Aspergillus or Asthma Causing the Mucus?
It’s often a combination — here’s how they can overlap:
| Condition | What It Might Do |
|---|---|
| Aspergillosis (e.g. ABPA or Aspergillus bronchitis) | Causes thick, sticky mucus with fungal elements and inflammation. Often leads to coughing up plugs or brown mucus. |
| Asthma | Can increase mucus production, especially if poorly controlled or if triggered by allergens (including Aspergillus). |
| Both together | May cause ongoing mucus, irritation, and airway narrowing that makes it harder to clear, despite constant coughing. |
If you're seeing more mucus than usual, it could mean:
-
A flare-up of fungal activity
-
A reaction to something environmental (e.g. pollen, dust, damp)
-
Or simply a bad asthma spell with more inflammation
🧼 The ‘Bottle Brush’ Analogy
An image of wanting to "scrub" the airways is very real — many describe the feeling of:
-
Something stuck that won’t budge
-
Needing a deep clean they can’t reach with coughing
-
Wishing there were tools to physically clear the airways
✅ What You Can Try to Help Clear the Mucus
Here are real methods people find helpful (with advice from a respiratory physio):
-
Airway Clearance Devices (like a ‘brush’ for your lungs!):
-
Flutter or Acapella devices: use vibration and pressure to loosen mucus
-
Positive Expiratory Pressure (PEP) therapy: helps open and clear airways
(You can ask your team for one, or see if your hospital physio provides them.)
-
-
Breathing & Huff Coughing Techniques:
-
Controlled deep breaths, then a huff (a strong open-mouthed exhale like steaming up a mirror) instead of hacking coughs
-
This moves mucus from deep down to the top of the lungs where it’s easier to shift
-
-
Positioning/Gravity Drainage (Postural Drainage):
-
Certain positions help drain mucus from different lobes of the lungs — especially useful for bronchiectasis or ABPA.
-
-
Steam with Caution:
-
Mild steam inhalation (e.g. from a shower) can loosen secretions — just avoid essential oils or herbs if you’re sensitive.
-
-
Hydration and Mucolytics:
-
Staying hydrated helps thin the mucus.
-
Some are prescribed carbocisteine to reduce mucus stickiness.
-
-
Speak to your team if:
-
The mucus is changing in colour or amount
-
You feel more breathless
-
You’re unsure if it’s a fungal flare or asthma spike
-
They might check for infection, offer a sputum test, or tweak your medication.
🗣️ Patient Voices
“I felt like I had cobwebs or glue in my lungs. The flutter device gave me back a sense of control — I still have to work at it, but I don’t feel as helpless.”
“When I learned to huff cough and did it properly, I was amazed at how much came up. It's not a miracle, but it made me feel cleaner inside.”