Other forms of aspergillosis:🌿 Allergic Fungal Rhinosinusitis (AFRS), A Complete Patient Guide
👃 What Is AFRS?
Allergic Fungal Rhinosinusitis (AFRS) is a rare, non-invasive allergic condition affecting the sinuses. It occurs when a person develops a strong allergic reaction to fungal spores — most often Aspergillus or other environmental moulds.
This allergic reaction causes:
-
Chronic sinus inflammation
-
Nasal polyps
-
Thick, sticky mucus (called allergic mucin)
-
Blocked sinus drainage
-
In some cases, bone changes due to pressure from the build-up
Importantly, the fungus does not invade tissues, unlike more serious forms of aspergillosis.
🧬 AFRS and ABPA: Similar Diseases in Different Places
AFRS is very similar in nature to Allergic Bronchopulmonary Aspergillosis (ABPA), which affects the lungs.
| Feature | AFRS | ABPA |
|---|---|---|
| Location | Sinuses (nose, face) | Lungs (airways) |
| Cause | Allergy to fungi (e.g. Aspergillus, Bipolaris) | Allergy to Aspergillus fumigatus |
| Type of condition | Allergic (non-invasive) | Allergic (non-invasive) |
| Main symptoms | Nasal blockage, thick mucus, polyps, facial pressure | Cough, wheeze, mucus plugs, breathlessness |
| Seen in | People with chronic rhinosinusitis, nasal polyps, allergic rhinitis | People with asthma or cystic fibrosis |
| IgE levels | Often raised | Typically >1000 IU/mL |
| Inflammatory cells | Eosinophils in sinus mucin | Eosinophils in sputum and blood |
| Treatment | Sinus surgery, nasal steroids, biologics (sometimes) | Oral steroids, antifungals, biologics (sometimes) |
🧠 In short:
AFRS is to the sinuses what ABPA is to the lungs — both are allergic responses to inhaled fungal spores.
In fact, some patients may have both conditions if fungal sensitivity affects multiple airways.
📉 How Common Is AFRS?
AFRS is uncommon, but may be underdiagnosed. It occurs mostly in people with long-standing sinus problems or fungal allergies.
| Group | Estimated prevalence |
|---|---|
| General population | Less than 1 in 10,000 |
| People with chronic rhinosinusitis | 5–10% |
| Sinus surgery patients | 6–9% |
| Humid climates (India, Southern US) | Up to 25–30% of CRS cases |
In the UK, AFRS is less common than in tropical areas — but awareness is growing.
🛑 Why Is It Often Missed?
-
Looks just like chronic rhinosinusitis with nasal polyps (CRSwNP)
-
Most patients have symptoms like blocked nose, facial pressure, and mucus
-
Doctors may treat these as routine infections without testing for fungal allergy
-
Diagnosis requires ENT, allergy testing, imaging, and often surgery
🧬 Who’s at Risk?
People most at risk of AFRS typically:
-
Have asthma, nasal polyps, or severe allergic rhinitis
-
Experience long-term or recurring sinus infections
-
Have elevated IgE levels or known allergies to fungi
-
Live in damp or mould-prone environments
-
May have other fungal allergic conditions, including ABPA
🧪 How Is AFRS Diagnosed?
Diagnosis is based on the Bent and Kuhn criteria, which include:
-
Chronic rhinosinusitis with nasal polyps
-
Characteristic "allergic mucin" seen on CT or during surgery
-
Positive fungal test (PCR or culture)
-
Evidence of IgE-mediated allergy (skin test or blood test)
-
CT scan showing sinus opacification, expansion, or bone thinning
A diagnosis is usually made by an ENT specialist, sometimes with support from allergists and microbiologists.
💊 Treatment and Management in 2025
1. Endoscopic Sinus Surgery (ESS)
-
Clears out mucin and polyps
-
Restores drainage and reduces symptoms
-
Often the first step in diagnosis and treatment
2. Nasal Corticosteroids
-
Long-term sprays or rinses to keep inflammation down
3. Short Courses of Oral Steroids
-
Reduce inflammation after surgery or during flare-ups
4. Biologic Medications
-
For recurrent or severe cases:
-
Anti-IgE (omalizumab)
-
Anti-IL-5 (mepolizumab, benralizumab)
-
Anti-IL-4/IL-13 (dupilumab)
-
5. Antifungals?
-
Not usually needed
-
Oral antifungals have not consistently helped in trials
🔁 Will It Come Back?
AFRS can recur, especially if polyps return or inflammation flares up. Most patients need ongoing care from an ENT team and occasional follow-up imaging or treatment adjustments.
✅ Key Takeaways
-
AFRS is a rare, allergic form of sinus disease caused by hypersensitivity to fungi like Aspergillus.
-
It shares similarities with ABPA, which affects the lungs.
-
It is non-invasive, but can be severe and persistent without treatment.
-
Diagnosis requires a combination of ENT evaluation, allergy testing, and imaging.
-
Most people improve with surgery, nasal steroids, and in some cases, biologic therapy.

🫁 Mucus Plugging in Aspergillosis: What It Is, Why It Happens, and What It Means
For patients with ABPA, CPA, Aspergillus bronchitis, or asthma
🔍 What Is a Mucus Plug?
A mucus plug is a thick clump of sticky mucus that becomes trapped in your lungs. It can block airways, cause coughing, and make breathing more difficult. In people with aspergillosis, this is common — but the type, location, and cause of the mucus can vary.
🧪 What Causes Mucus Plugging?
Your lungs naturally make mucus to protect against germs and irritants. But in fungal or allergic lung disease, this mucus may:
-
Be produced in excess
-
Become too thick or sticky
-
Get trapped due to airway damage
Aspergillosis-related causes include:
-
ABPA (Allergic Bronchopulmonary Aspergillosis) – inflammation causes thick, sticky mucus
-
Aspergillus bronchitis – fungus lives in mucus, producing biofilms
-
CPA (Chronic Pulmonary Aspergillosis) – may lead to mucus due to structural damage
-
Bronchiectasis – airways are widened and can no longer clear mucus properly
🧬 Are All Mucus Plugs the Same?
No. Mucus plugs vary in colour, texture, cause, and treatment. Here's how they differ:
| Type of Plug | What You Might See | What It Could Mean | Common in... |
|---|---|---|---|
| Sticky, stringy | Clear/yellow, like glue | Allergic inflammation | ABPA, asthma |
| Rubbery or solid | Brown, rubbery, “slug-like” | Allergic + fungal mix | ABPA, Aspergillus bronchitis |
| Green or smelly | Thick, foul-smelling | Infection (bacteria) | Bronchiectasis |
| Foamy or frothy | Clear/white, bubbly | Non-infectious irritation | COPD, asthma |
| Black or speckled | May contain fungal specks | Fungal growth | CPA, fungal bronchitis |
🖼️ What Do Mucus Plugs Look Like on a CT Scan?
Below are real examples of CT scan findings showing mucus plugging in different forms of aspergillosis and related conditions.
🧷 1. Finger-in-glove sign (ABPA)
Mucus in large airways appears like fingers inside a glove. This is common in allergic fungal airway disease.
➡ Seen in: ABPA, bronchiectasis with fungal colonisation
📍 Note: Branching tubular opacities filled with mucus.
🌿 2. Tree-in-bud pattern
Small airway blockage — plugs in the tiniest branches of the lungs. Common in infection, inflammation, and Aspergillus bronchitis.
➡ Seen in: Aspergillus bronchitis, asthma, CPA with superinfection
📍 Note: Tiny dots and lines in a tree-like shape.
🧱 3. Lung collapse (atelectasis) from plug
A large mucus plug can block a main airway, causing collapse of part of the lung.
➡ Seen in: Severe ABPA, CPA, patients with weakened cough reflex
📍 Note: Whiteout of part of lung where plug is blocking airflow.
📸 Example CT Findings

1. Bronchiectasis + mucus plug
Area in the left lower lung shows dilated bronchi filled with mucus—classic for bronchiectasis with mucoid impaction

2. Extensive bronchiectasis with plugs
Widespread thick-walled airway dilatation accompanied by mucus plugs (black arrows) and consolidation (black arrowheads)

3. Luminal plugging in small airways
Subtle luminal opacities in peripheral bronchi—the “tree‑in‑bud” pattern common in asthma, COPD, and infections.

4. Atelectasis (part of the lung has collapsed or isn’t fully inflating) due to mucus plugging
Consolidation and small airway blockage leading to lung collapse, highlighted by arrows in the upper lobe.
💡 Clinical Takeaways
| Feature | What it indicates |
|---|---|
| Mucoid impaction | Large airway fungal/allergic plugs (e.g., ABPA) or bronchiectasis |
| Tree‑in‑bud | Small-airway infection/inflammation (e.g., TB, PCD, asthma) |
| Atelectasis | Complete blockage, leading to collapse and consolidation |
| Persistent luminal plugs | Associated with worse airflow obstruction and symptoms in COPD/asthma |
✅ Next Steps / Applications
-
These CT examples are valuable for educational use—they illustrate the different patterns seen in mucus plugging across disease types.
-
Radiologists often use these signs to help diagnose and tailor management (infection, allergy, structural lung disease).
-
If your patients or students need simplified visuals, these scans paired with annotations (e.g., arrows, labels) can make great teaching tools.
🧠 What Does It Feel Like?
People often say:
“It felt like something was stuck and wouldn’t come out.”
“I finally coughed up a rubbery strand — like glue.”
“Once it cleared, I could breathe better instantly.”
🧼 How Are Mucus Plugs Treated?
Treatment depends on the underlying cause:
✅ Medications
-
Steroids – reduce inflammation in ABPA and asthma
-
Antifungals – lower fungal load (e.g., itraconazole, posaconazole)
-
Mucolytics – thin mucus (e.g., carbocisteine, hypertonic saline)
-
Antibiotics – treat bacterial infections
✅ Airway Clearance Techniques
-
Respiratory physio – helps you learn how to shift mucus
-
Devices – flutter valve, PEP mask, Acapella
-
Inhaled/nebulised therapy – opens airways and loosens plugs
⚠️ Always speak to your clinical team before starting a new technique.
🧪 Can Coughing Up a Plug Help Diagnosis?
Yes! If you cough up a rubbery, large, or unusual plug, it can be:
-
Tested for fungus, bacteria, or allergy cells (eosinophils)
-
Sent for culture to detect Aspergillus
-
Helpful in guiding or confirming diagnosis of ABPA or Aspergillus bronchitis
👣 Key Points for Aspergillosis Patients
| Question | Answer |
|---|---|
| Is mucus plugging common? | Yes, especially in ABPA, CPA, and bronchiectasis |
| Are all mucus plugs the same? | No – they vary in size, shape, colour, and cause |
| What should I do if I cough one up? | Tell your doctor – it may be useful to test |
| Can it be seen on scans? | Yes – CT can show where plugs are and how severe |
| Can it be treated? | Yes – treatments include steroids, antifungals, mucolytics, and physio |
👁️ Other forms of Aspergillosis: Aspergillus Endophthalmitis, A Rare Eye Infection
🧐 What Is It?
Aspergillus endophthalmitis is a severe fungal infection that affects the inside of the eye — specifically the vitreous (gel) or retina — caused by Aspergillus. It can lead to:
-
Red, painful eye
-
Blurred or lost vision
-
Eye inflammation, sometimes with “filamentous” fungal growth on the lens if post-surgery
-
Both exogenous (from cataract surgery or injury) and endogenous (spread through the blood, often in immunocompromised patients) forms exist
📉 How Rare Is It?
| Condition | Cases per 100,000 | Commonality |
|---|---|---|
| ABPA | 40–60 | Moderately common |
| CPA | 3–4 | Uncommon |
| Aspergilloma | 0.5–1 | Rare |
| Empyema | <0.1 | Very rare |
| Endocarditis | <0.05 | Extremely rare |
| Endophthalmitis | Estimated < 0.05 | Extremely rare |
-
Aspergillus causes fewer than 1% of postoperative eye infections
-
Even among fungal cases, it’s a leading but still uncommon cause
🧬 Who Is at Risk?
-
Immunocompromised individuals (e.g., transplant, high-dose steroids, cancer infusion, diabetes, HIV)
-
Post-operative or post-trauma eye patients, especially cataract surgery
-
IV drug users, or people with systemic aspergillosis
Despite these risk factors, it remains an uncommon complication.
🩺 Symptoms
-
Eye pain and redness
-
Blurry or reduced vision
-
Sensation of “floaters” or shadows
-
Often unilateral, but can be bilateral, especially after surgery or in immunosuppressed patients
🧪 Diagnosis
-
Eye examination by an ophthalmologist with slit lamp or ultrasound
-
Sampling of vitreous or aqueous fluid for culture, PCR, or galactomannan tests
💊 Current Treatment Guidelines
Based on 2022–2025 evidence:
-
Prompt vitrectomy (surgical removal of infected gel) improves outcomes Intravitreal voriconazole injections (directly into the eye) enhance recovery
-
Systemic antifungals: voriconazole or isavuconazole are preferred; amphotericin B or combination therapy may be used if resistant
-
Prognosis: Vision ≥20/400 in <50% of cases; globe preserved in ~66% of eyes
🧭 Summary for Patients
-
Aspergillus endophthalmitis is extremely rare — it affects a tiny fraction of aspergillosis patients.
-
It’s often linked to eye surgeries, trauma, or severe immunosuppression.
-
Symptoms include pain, redness, floaters, and vision loss — if any appear, seek urgent ophthalmology care.
-
Best outcomes result from early vitrectomy, intravitreal antifungals, and systemic treatment.
✅ Bottom Line
While Aspergillus can affect many parts of the body, eye infections (endophthalmitis) are among the rarest forms. Most patients with respiratory forms (ABPA, CPA, or aspergilloma) will never develop this.
But awareness matters — especially for those who are immunocompromised or have had eye surgery. With swift, specialist treatment, many eyes can be saved, though vision recovery is often limited.
❤️🩹 Other forms of Aspergillosis: Aspergillus Endocarditis, Understanding a Rare Heart Infection
🫀 What Is It?
Aspergillus endocarditis is a rare infection of the heart’s inner lining (endocardium) caused by the fungus Aspergillus. This condition affects the heart valves (native or prosthetic), the inner wall of the heart, or even devices such as pacemaker leads. The fungus forms large masses called vegetations and can spread to the brain or other organs.
📉 How Rare Is It?
This is among the rarest forms of aspergillosis:
| Type of Aspergillosis | Estimated Cases per 100k | Commonality |
|---|---|---|
| ABPA | 40–60 | Moderately common |
| CPA | 3–4 | Uncommon |
| Aspergilloma | 0.5–1 | Rare |
| Aspergillus Empyema | <0.1 | Very rare |
| Aspergillus Endocarditis (AE) | <0.05 | Extremely rare |
⚠️ Who Is at Risk?
AE usually occurs in individuals who:
-
Are immunocompromised (e.g., cancer chemotherapy, transplant recipients, high-dose steroids)
-
Have heart valve abnormalities or a prosthetic valve
-
Had cardiac surgery or devices placed
-
Are critically ill or have severe fungus in the bloodstream
Even with these factors, AE remains extremely uncommon, but its rapid progression makes awareness and early treatment crucial.
🩺 How It’s Diagnosed
Diagnosis is challenging due to:
-
Negative blood cultures (blood tests usually don’t detect Aspergillus)
-
Symptoms often include fever, new heart murmur, or emboli (e.g., stroke)
-
Echocardiograms (TTE/TEE) may reveal large vegetations or abscesses
-
Valve or embolus tissue tested via PCR or galactomannan confirms diagnosis
⏳ Prognosis
-
AE has a very high mortality rate, ranging from 50–90%, often due to delayed diagnosis
-
Even with treatment, survival is around 50–60% with surgery and antifungals; without surgery, survival falls below 5–10%
💊 Current Treatment Guidelines
🛠️ 1. Early Surgical Intervention + Antifungal Therapy
-
Surgery to remove infected tissue and replace valves is essential
-
Voriconazole (an antifungal) is the preferred medication; liposomal amphotericin B is an alternative
-
Combined therapy (two antifungals) may improve outcomes in certain cases
🕰️ 2. Long-Term or Lifelong Antifungal Treatment
-
Lifelong antifungals may be needed to prevent recurrence, especially when prosthetic valves are involved
🧪 3. Monitoring and Follow-Up
-
Regular monitoring through clinical exams, echocardiograms, and possibly biomarkers
-
Watch for signs of relapse or emboli (e.g., neurological symptoms)
📘 Case Insights
-
A patient with a prosthetic aortic valve had ≥60% survival with surgery + voriconazole and long-term suppressive treatment
-
Another recovered from native valve involvement with combined antifungal therapy and surgery, despite being previously healthy
-
Without surgery and antifungals, AE is almost always fatal — mortality approaches 100%
✅ What This Means for Patients
-
AE is extremely rare, particularly compared to other forms like ABPA or CPA.
-
It occurs mostly in people with significant risk factors — immunosuppression, prior heart surgery, or invasive devices.
-
If suspected, early recognition and referral to a specialist center is urgent.
-
Treatment combines surgery and antifungals, and usually requires long-term care.
🧭 Bottom Line
Aspergillus endocarditis is a serious and rare complication. While most people with aspergillosis (like ABPA or CPA) will never develop it, anyone with heart valve issues and severe immune weakness should be vigilant.
With early, specialist treatment, recovery is possible — but only if the condition is identified and treated quickly.
When Antifungals Fail: One Patient’s Recovery from Subacute Invasive Aspergillosis After Surgery
Subacute Invasive Aspergillosis (SAIA) is a rare and serious lung infection caused by the Aspergillus fungus. It often affects people who are immunocompromised—whether due to illness or medications like immunosuppressants—and typically sits between chronic and acute invasive forms in severity.
🧬 A Patient's Story from Australia
“I was diagnosed with SAIA after being treated with immunosuppressants for an autoimmune condition. Over seven months, I tried three different antifungal medications—but the infection persisted. I was still producing thick mucus and felt systemically unwell, almost like I had a constant infection running through me.
Four weeks ago, I underwent a wedge resection—a type of surgery where the affected part of my lung was removed. Since then, my symptoms have completely resolved. I’m no longer coughing or feeling septic.
My infectious diseases specialist plans to keep me on posaconazole for 12 months, with monthly galactomannan blood tests to catch any recurrence early.
I’ve found there’s very little published about surgery for SAIA, so I hope my experience might help others.”
🧪 What Is SAIA?
SAIA is a slowly progressive lung infection that develops over weeks to months. Unlike acute invasive aspergillosis, which moves quickly, SAIA often occurs in people with some degree of immune suppression but who aren’t completely immunocompromised.
It can present with:
-
Persistent cough
-
Low-grade fever
-
Fatigue
-
Mucus production
-
Progressive lung damage
Standard treatment involves long-term antifungal therapy, often with drugs like:
-
Itraconazole
-
Voriconazole
-
Posaconazole
But in some cases—like this patient’s—antifungal therapy alone isn’t enough.
🛠️ When Is Surgery Used for SAIA?
Surgery, including wedge resection, may be considered when:
-
Antifungal medications are not effective
-
The infection is localized to one part of the lung
-
There is persistent or worsening lung damage
-
Patients are fit enough to undergo surgery
🔍 What Does the Evidence Say?
Although not commonly performed, surgery for aspergillosis is documented in medical literature, especially in cases of:
-
Chronic pulmonary aspergillosis (CPA)
-
Fungal nodules
-
Subacute forms like SAIA
Key studies:
-
A U.S. study of >100,000 aspergillosis cases found that only 4.8% underwent surgery, usually for treatment failure or severe complications.
-
A Chinese study of 85 CPA patients showed a relapse rate of only 7% post-surgery, with most patients improving dramatically.
-
A UK case series described 30 patients having lung resections over 15 years, showing surgery is safe and effective when performed in experienced centres.
🔄 What Happens After Surgery?
Even after a successful resection, follow-up antifungal treatment is often continued to prevent recurrence. Monitoring usually includes:
-
Regular imaging (CT scans)
-
Galactomannan blood tests (to detect fungal components)
-
Symptom tracking
This is typically guided by a multidisciplinary team involving infectious diseases, respiratory, and thoracic surgery specialists.
🎯 Key Takeaways
-
SAIA is uncommon, and when antifungals fail, surgery can be life-changing.
-
Wedge resection is a lung-sparing procedure that removes just the infected portion, offering good outcomes when the disease is localised.
-
Ongoing antifungal therapy and monitoring are critical to long-term success.
-
Your story adds to a growing but still limited body of knowledge and may help inform future treatment decisions and encourage further research.
If you are a patient or clinician navigating SAIA and struggling with antifungal treatment, this story may offer hope—and a reminder that surgical options, though rarely needed, can be effective when used judiciously.
🧵 Why Am I Getting More “Plugs” This July?
A message for aspergillosis patients
July is often a time when people with aspergillosis feel a bit better — but sometimes, things don’t go quite to plan. If you’ve suddenly started getting more mucus “plugs” or are struggling to clear your chest, here are some possible reasons:
🔍 Common Reasons for More Mucus or Plugs in Summer
| Possible Cause | Why it might affect you now |
|---|---|
| Fungal spores are high | July and August bring very high outdoor levels of Aspergillus, Cladosporium, and other moulds – especially on dry, windy days or after cutting grass. These can trigger inflammation and more mucus. |
| Pollen season continues | Even though tree pollen has gone, grass, weed, and cereal pollen are still in the air. These can worsen symptoms for people with ABPA or asthma. |
| Humidity or storms | Sudden weather changes, humid air, or storms can make breathing more difficult and mucus harder to shift. Some people call this "thunderstorm asthma." |
| Air pollution (ozone) | Sunny weather increases ozone and air pollution – both can irritate your airways. |
| Low-level infection or flare-up | If your mucus is thicker, darker, or smells different, it might be a sign of a fungal or bacterial flare-up, even without a high temperature. |
| Hydration or medication changes | Less water, skipping nebulisers, or changes in routine can make mucus stickier. |
| Blocked sinuses | Post-nasal drip from fungal sinusitis can make it feel like mucus is always sitting in your throat or upper chest. |
✅ What You Can Do
-
Drink more fluids, especially warm water or squash
-
Use saline in your nebuliser to loosen thick mucus
-
Do your chest clearance exercises more often – flutter device, ACBT, or huffing
-
Don’t skip antifungals, inhalers, or mucolytics like carbocisteine
-
Consider a nasal rinse if your sinuses feel blocked
-
Keep windows closed on high spore or high pollen days
-
Speak to your team if things don’t settle – you may need a review or antibiotics
⚠️ When to Get Checked
-
You're coughing up yellow, green or brown mucus
-
Mucus smells bad or has blood in it
-
You feel more breathless or more tired
-
You’ve needed to increase your nebuliser use
💬 You're Not Alone
Many patients with aspergillosis get more mucus at this time of year — even when the sun’s out! Don’t assume it’s “just the weather.” Sometimes it’s a sign that your lungs or sinuses are reacting to invisible spores in the air.
Other forms of aspergillosis: Aspergillus Empyema, A Rare and Serious Complication of Aspergillosis
What Is Aspergillus Empyema?
Aspergillus empyema is a very rare but serious fungal infection where Aspergillus invades the pleural space — the thin cavity between the lungs and the chest wall. Normally, this space contains a small amount of lubricating fluid. In empyema, it fills with infected pus, often due to rupture from a lung cavity or complication following severe illness or surgery.
In this form of aspergillosis, the infection goes beyond the lungs into the lining around the lungs (pleura), and is typically seen in people with severe underlying lung disease or who are very immunocompromised.
How Rare Is It?
| Type of Aspergillosis | Estimated Cases per 100,000 People | How Common? | Who Is Most at Risk? |
|---|---|---|---|
| ABPA (Allergic Bronchopulmonary Aspergillosis) | ~40–60 | Moderately common | People with asthma or cystic fibrosis |
| CPA (Chronic Pulmonary Aspergillosis) | ~3–4 | Uncommon | People with underlying lung disease (e.g. TB, COPD) |
| Aspergilloma (fungus ball) | ~0.5–1 | Rare | People with lung cavities (often overlaps with CPA) |
| Aspergillus Empyema | < 0.1 | Very rare | Severely immunocompromised or critically ill ICU patients |
Most people living with ABPA or CPA will never develop Aspergillus empyema.
Who Is at Risk?
Risk of empyema increases in people who have:
- Severely weakened immune systems (e.g. high-dose corticosteroids, cancer treatment, transplant)
- Lung surgery, trauma, or chest drain procedures
- A ruptured aspergilloma (fungus ball)
- Existing lung cavities (from TB, sarcoidosis, or CPA)
- Severe COVID-19 or ARDS (acute respiratory distress syndrome) with damaged lung tissue
Even among high-risk patients, Aspergillus empyema remains rare.
Symptoms
- Fever that does not improve with antibiotics
- Chest pain or tightness
- Breathlessness
- Cough (may be foul-smelling)
- Persistent fluid seen on chest X-ray or CT scan
Diagnosis
Doctors may use:
- CT scans or chest X-rays to detect fluid or cavities
- Pleural fluid sampling (for fungal culture, galactomannan, PCR)
- Tissue biopsy in difficult or unclear cases
Treatment Options
1. Drain the Infected Fluid
- Chest drain (tube)
- Surgical drainage in complex cases
2. Antifungal Therapy
- Usually voriconazole (oral or IV)
- Treatment may last months, depending on response
3. Surgery
- May include decortication (removing infected pleura)
- Repair of fistulas or ruptured cavities
- Muscle or fat flaps to prevent recurrence and close space
4. Other Measures (used selectively)
- Intrapleural antifungal instillation (amphotericin)
- Endobronchial valves or spigots to manage air leaks
Outcomes and Prognosis
- Historically high mortality (30–75%), mostly due to delayed diagnosis or underlying illness
- Outcomes improving with specialist antifungal and surgical treatment
- Early intervention saves lives
Summary for Patients
- Aspergillus empyema is very rare, and affects only a tiny number of people with aspergillosis — usually those who are very unwell, immunocompromised, or post-surgery.
- It is treatable with antifungals, drainage, and sometimes surgery.
- Most people with ABPA or CPA will never experience this complication.
- Stay aware of symptoms, and ensure regular check-ups if you have known lung cavities or risk factors.
Other forms of aspergillosis: 🛡️ Tracheobronchial Aspergillosis (TBA), A Rare Airway Form of Aspergillus Infection
🌿 What is Tracheobronchial Aspergillosis?
Tracheobronchial aspergillosis (TBA) is a rare type of aspergillosis that affects the large airways (the trachea and bronchi), rather than the deeper parts of the lungs. It happens when Aspergillus, a common environmental mould, starts to grow in the airways, either sitting in mucus or, in severe cases, invading the airway wall itself.
❗How Rare Is It?
TBA is uncommon — even among people who already have aspergillosis.
It is mostly seen in:
-
Very unwell hospitalised patients
-
People with severe immune suppression
-
Patients in intensive care units (ICU)
🧠 If you have ABPA, CPA, asthma, or chronic sinus issues, your risk of developing TBA is usually very low, unless your immune system becomes severely weakened.
🔍 What Causes It?
The Aspergillus fungus is found everywhere — but in some people with weak defences, it can take hold in the airways. Depending on the type and severity, this can cause:
-
Thick fungal mucus or plugs in the airways
-
Persistent coughing or wheezing
-
Breathlessness
-
In serious cases, damage to the airway lining or even bleeding
🚨 Who Is Most at Risk?
People most at risk of invasive or serious TBA include those who are:
| High-Risk Group | Why They're at Risk |
|---|---|
| ICU patients on ventilators | Damaged airways + suppressed local immunity |
| Patients with severe viral pneumonias (e.g. COVID-19, influenza) | Airways inflamed and vulnerable |
| Stem cell or organ transplant recipients | Profound immune suppression |
| Cancer patients undergoing chemotherapy | Low white blood cells (neutropenia) |
| People on high-dose steroids or immunosuppressants | Weakens the body's response to fungal growth |
| People with COPD or bronchiectasis in critical care | Pre-damaged airways and infection risk |
🧬 What About People with CPA, ABPA, or Asthma?
Many people living with:
-
Chronic Pulmonary Aspergillosis (CPA)
-
Allergic Bronchopulmonary Aspergillosis (ABPA)
-
Asthma with fungal sensitisation (SAFS)
…may worry that Aspergillus in their lungs or sinuses could spread to their airways.
🟢 Good news: TBA is not common in these groups unless:
-
You become severely immunocompromised (e.g. after a transplant or due to high-dose steroids)
-
You are admitted to ICU or receive strong immunosuppressive therapy
If you are on replacement doses of steroids (e.g. for adrenal insufficiency) or biologics for asthma, your risk is generally low, especially if you are also on antifungal treatment when needed.
🧪 How Is TBA Diagnosed?
Doctors may consider TBA if someone at risk develops:
-
New or worsening cough
-
Mucus that won’t clear
-
Breathing difficulties
-
Signs of bleeding in the airways
Diagnosis may involve:
-
Bronchoscopy (looking into the lungs with a camera)
-
Bronchoalveolar lavage (BAL) to test for Aspergillus DNA or galactomannan
-
CT scans of the chest
💊 How Is TBA Treated?
Treatment depends on whether the infection is simply growing in mucus or is invading tissue:
| Type of TBA | Treatment |
|---|---|
| Fungal growth in mucus only | Bronchoscopic removal of plugs ± antifungals if immunocompromised |
| Inflammation of airway lining | Oral or inhaled antifungals, possibly systemic therapy if symptoms persist |
| Tissue-invasive TBA | Urgent treatment with voriconazole or isavuconazole, often for 6–12 weeks; sometimes with amphotericin or an echinocandin |
✅ Summary for Aspergillosis Patients
| Question | Answer |
|---|---|
| Is TBA common? | ❌ No — it is rare |
| Who usually gets it? | ICU patients, transplant recipients, cancer patients, or those with severe immune suppression |
| Can people with CPA or ABPA get TBA? | 🟠 Possibly — but only if their immunity becomes severely weakened |
| Are replacement steroids or asthma biologics risky? | 🟢 Not usually — especially if antifungal cover is used when needed |
| Is it treatable? | ✅ Yes — if caught early and treated appropriately with antifungals |
🧠 Final Advice
If you have any form of aspergillosis, it's important to work closely with your clinical team. Most people will never develop TBA. But if you are on strong immune-suppressing treatment or become very unwell in hospital, make sure your team is aware of your history. With careful monitoring and the right treatment, outcomes can be good.
🛡️ Understanding Your Risk: Aspergillosis, Steroids, and the Immune System
If you’ve been diagnosed with an Aspergillus-related condition, such as chronic pulmonary aspergillosis (CPA), ABPA, or a fungal ball (aspergilloma), you might wonder:
“Am I immunocompromised? And do steroids or biologics put me at more risk?”
The answers depend on your underlying health, medications, and how your body responds to Aspergillus.
🌍 Aspergillus is Common — But Not Harmless
Aspergillus is a type of mould found everywhere — in soil, air, and dust. Most people breathe it in daily without problems. But in some people, it can:
-
Trigger an allergic reaction (ABPA or fungal sinusitis)
-
Cause infection in damaged lungs (CPA or aspergilloma)
-
Spread aggressively in those with very weak immune systems (invasive aspergillosis)
Understanding your level of immune defence helps explain your risk and how your treatment should be managed.
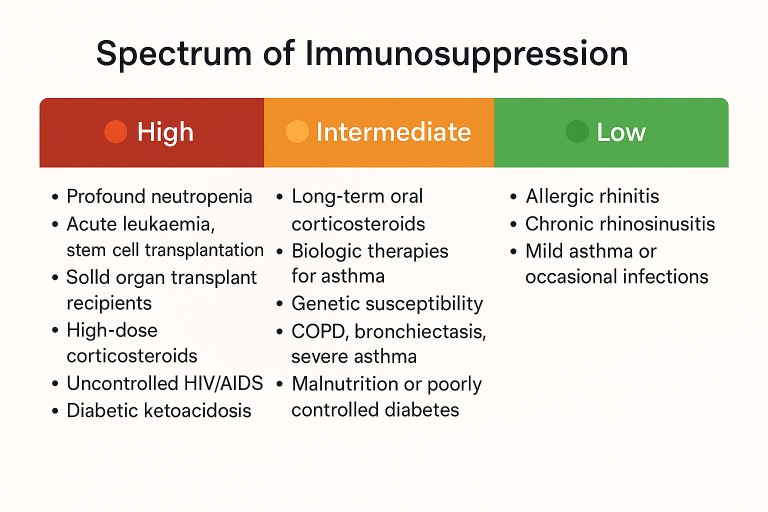
🧬 Levels of Immunocompromise: What They Mean
Immunosuppression isn't black-and-white — it's a spectrum. Here's how it applies to people with or at risk of aspergillosis:
🔴 High-Level Immunosuppression (High Risk)
-
Recent chemotherapy or bone marrow transplant
-
Stem cell or organ transplant
-
Severe neutropenia (very low white blood cell count)
-
High-dose steroids (e.g. ≥20 mg prednisolone daily for weeks)
-
Uncontrolled HIV/AIDS
-
Intensive care or mechanical ventilation
🧠 These people are at risk of serious, fast-spreading infections — including invasive aspergillosis (IA), which is rare but life-threatening.
🟠 Moderate Immunosuppression (Common in Aspergillosis Patients)
-
Long-term low-to-moderate steroids (e.g. <10–15 mg prednisolone)
-
Biologics for asthma (e.g. omalizumab, benralizumab)
-
Chronic lung disease (COPD, bronchiectasis, asthma)
-
Diabetes, malnutrition, or genetic immune traits
-
Previous TB, sarcoidosis, or other lung damage
🧠 This group is at greater risk of chronic forms of aspergillosis — especially CPA, ABPA, and aspergillus bronchitis.
🟢 Low or No Immunosuppression (Low Risk)
-
People with well-controlled asthma or sinusitis
-
Those on occasional short courses of steroids
-
No major lung or immune conditions
🧠 This group is unlikely to develop aspergillosis.
💊 What if You Already Have Aspergillosis?
If you’ve been diagnosed with CPA, ABPA, aspergilloma, or sinus disease caused by Aspergillus, some treatments may still increase your vulnerability if not carefully managed.
❗ Steroids (e.g. Prednisolone)
-
Help control inflammation (especially in ABPA)
-
But also suppress immunity, making it easier for Aspergillus to grow
-
Can worsen CPA or increase risk of bleeding in aspergilloma
-
Risk rises with higher doses and longer courses
🟠 If steroids are needed, they should usually be combined with antifungal medication (like itraconazole or voriconazole) to keep fungal growth in check.
❗ Biologics for Asthma (e.g. Omalizumab, Mepolizumab)
-
Target allergic inflammation without broadly suppressing the immune system
-
Don’t usually increase the risk of invasive fungal infections
-
May slightly alter how your immune system responds to Aspergillus
🟠 Biologics can be helpful in ABPA and severe asthma, but regular monitoring is still important.
🔍 Summary Table: Common Risk Factors and What They Mean
| Factor | What It Does | What to Watch For |
|---|---|---|
| Long-term steroids | Suppress immune cells, reduce inflammation | Use with antifungals; monitor closely |
| Biologics for asthma | Modulate immune pathways (e.g. IgE, IL-5) | Safe in most; watch for subtle effects |
| TB, sarcoid, or other lung scarring | Leaves cavities that allow fungal growth | Regular scans and blood tests |
| Diabetes or malnutrition | Affects immune function and tissue repair | Keep well-managed |
| Low white blood cells (neutropenia) | Limits ability to fight fungal infection | Urgent action needed if fever or unwell |
| Lung diseases (COPD, asthma, bronchiectasis) | Reduce local lung defences | Increases risk of CPA, ABPA, or colonisation |
✅ What Can You Do to Stay Safe?
-
Take antifungals as prescribed, especially if you're on steroids or biologics
-
Avoid unnecessary long-term steroid use — use the lowest dose for the shortest time
-
Report new or worsening symptoms early — especially breathlessness, coughing blood, fatigue, or sinus pain
-
Have regular follow-ups with your respiratory or infectious diseases team
-
Don’t stop any medication suddenly — especially steroids — without medical advice
💬 Final Reassurance
Having aspergillosis doesn’t mean you’re severely immunocompromised — but some treatments can increase your risk if not managed carefully. With the right balance of antifungals, asthma treatments, and medical support, many people live well with ABPA, CPA, and related conditions.
Other forms of Aspergillosis
The majority of patients with aspergillosis will have forms that affect their lungs, as of course, that is where most exposure to Aspergillus occurs when we inhale the spores. There are, however, many more areas of our bodies that can be infected with Aspergillus. The sites of infection are much more difficult for spores to reach, so these forms of aspergillosis are much rarer compared with pulmonary forms, but they do occasionally happen, and as this is a website concerned with all forms of aspergillosis, we will try to summarise each form in this series of articles.
If you have been diagnosed with one of these rarer forms of aspergillosis you are welcome to join our support groups on Facebook, but be sure to explain which form you have, in any questions that you may ask, to avoid confusion. Different forms of aspergillosis can be treated in very different ways so be sure that the information you read is relevant to your aspergillosis.
There has long been a listing of other forms of aspergillosis in the treatment section of the Aspergillus & Aspergillosis website. These articles are intended for medical specialists so we will attempt to interpret them here for patients & non-specialists and also provide updated information where appropriate.
- Acute Invasive Aspergillus Sinusitis (AIAFS)
- Airways (tracheobronchial)
- Aspergillus Empyema
- Aspergillus Endocarditis