Airway Clearance, Diagnosis & Physiotherapy

Exercise and Aspergillosis: How Physical Activity Can Improve Breathing, Strength and Wellbeing
Last reviewed: June 2026 Key…


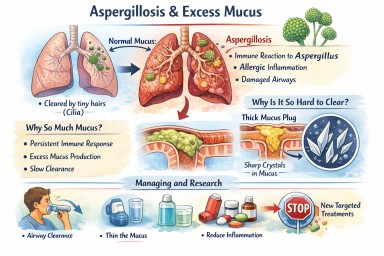



🫁 Mucus Plugging in Aspergillosis: What It Is, Why It Happens, and What It Means
For patients with ABPA, CPA,…

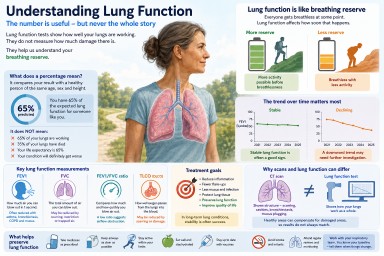
🫁 Understanding Bronchiectasis, COPD, and Aspergillosis: What Patients Need to Know
Living with a lung condition…