
Drug Safety in the UK: What Aspergillosis Patients Need to Know
Living with aspergillosis often means taking powerful medicines for a long time — antifungals, steroids, antibiotics, or even biologics. These treatments can be life-saving, but they can also cause side effects, especially when used together. It’s natural to wonder: How do we know these drugs are safe? What happens if something goes wrong?
This article explains how drug safety is managed in the UK, what happens when rare problems occur, and what resources patients can use to protect themselves.
How Medicine Safety Works
Before a drug is approved:
Every new medicine goes through several phases of clinical trials. These trials are not just about proving that the drug works (efficacy) — they are also about proving it is safe enough to use in people. Researchers record every possible side effect, monitor blood tests, and look for safety signals as well as improvements in the illness.
However, trials have limits. They usually include only a few thousand participants, so they can reliably detect common side effects but not very rare ones. For example, if a side effect happens in 1 in 100,000 people, and a trial only studies 50,000, it may not appear at all.
After a drug is approved:
Once a medicine is prescribed to thousands or millions of people, those rare side effects start to appear. For example, in the first million patients, perhaps 10 cases may be reported. That’s not manipulation — it’s just the maths of large numbers.
How Do Doctors Link a Side Effect to a Medicine?
When someone develops a new symptom, it isn’t always obvious whether it’s caused by their illness, another condition, or the medicine they’re taking. Linking a side effect to a drug usually involves several steps:
-
Timing – Did the symptom start soon after beginning the medicine? Did it improve when the medicine was stopped? Timing is often the strongest clue.
-
Known side effect profile – Doctors check if the symptom has been reported before in trials, studies, or drug safety updates.
-
Other explanations – Could it be the underlying condition (like aspergillosis) or another drug? All possible causes are reviewed.
-
Drug interactions – Many side effects come from the way medicines interact, rather than one drug alone. Antifungals like itraconazole and voriconazole interact with steroids, antibiotics, and heart drugs.
-
Rechallenge (rarely used) – Sometimes a drug is restarted to see if the side effect returns. This can provide strong evidence but is only done when absolutely necessary.
-
Patient reporting – A single case may not prove much, but when dozens of patients report the same issue, patterns become clear.
🔎 Key message: It’s not always quick or simple to prove a side effect. That’s why your own observations — when it started, how it feels, what other medicines you’re on — are so valuable to your doctors and to the Yellow Card system.
What Happens to Those Patients?
-
Every case is recorded and investigated. Regulators like the MHRA (Medicines and Healthcare products Regulatory Agency) look for patterns.
-
If a link is confirmed, they can issue warnings, add monitoring requirements, restrict use, or withdraw the drug.
-
For the patients affected, the drug is usually stopped, and supportive treatment is given. Sadly, in some cases, harm cannot be reversed.
This is why reporting side effects is so important. Each individual case helps build the full safety picture and protects others in the future.
Is This “Experimenting on Patients”?
It can sometimes feel that way — because new medicines are still watched closely after approval, and some harms are only seen later.
But there’s an important distinction:
-
Clinical trials are the experiments, and they are about safety as much as efficacy. Every trial phase collects safety data, and a medicine cannot be approved unless it is shown to be safe enough for use.
-
Post-marketing monitoring is not an experiment — it’s a safety net that exists for all medicines, because no trial is ever large enough to catch every very rare problem.
Patients aren’t being experimented on after approval, but your experience does matter. Every report adds to knowledge and helps keep medicines safe for everyone.
Who Is Liable If Harm Occurs?
-
Negligence (e.g. wrong dose, ignoring abnormal tests): the prescriber or hospital may be liable.
-
Defective product or hidden data: the manufacturer may be held responsible, sometimes through compensation schemes or legal action.
-
Very rare, unpredictable events despite correct use: liability is often less clear, and compensation is not guaranteed.
This can feel unfair. A few patients may suffer harm without anyone being “at fault.” That’s why strong safety monitoring and reporting are so essential.
Balancing Benefit and Risk
If 10 people out of a million are harmed, 999,990 people may have been helped — often in life-saving ways. That doesn’t make the harm any less real, but it explains why regulators still approve medicines with very rare risks: the benefit to the vast majority outweighs the small chance of harm, as long as those harms are recognised and acted on quickly.
Looking forward, science may allow us to predict who is at risk of those 1-in-a-million harms (through genetics or biomarkers) and screen them out — so that only those who can benefit safely receive the drug.
Key UK Drug Safety Resources
Here are the most useful resources for patients in the UK:
-
Yellow Card Scheme – report any suspected side effect or device problem. Patients, carers, and clinicians can all use it.
-
MHRA – the government body that regulates medicines and devices, publishes safety updates.
-
NHS Medicines A–Z – patient-friendly information on most drugs, including side effects.
-
Electronic Medicines Compendium (eMC) – official patient information leaflets for every licensed UK medicine.
-
British National Formulary (BNF) – the prescribers’ reference, also viewable by patients.
What Aspergillosis Patients Need to Remember
Because aspergillosis often requires long-term, powerful medicines like itraconazole, voriconazole, posaconazole, steroids, or biologics, patients are more likely to:
-
Experience side effects
-
Need regular blood tests to check drug levels
-
Take multiple medicines with possible interactions
Three key takeaways:
-
Know where to look – check NHS Medicines A–Z or your medicine leaflet (eMC) if you’re unsure about a side effect.
-
Report problems – use the Yellow Card scheme to flag any suspected reaction.
-
Stay in touch with your team – never stop or change your medicine without advice, but do share new symptoms with your GP or specialist promptly.
✅ Bottom line: Clinical trials test both safety and effectiveness, but no study can capture every rare event. That’s why medicines continue to be monitored after approval, and why patient reporting is so important. By working together — patients, doctors, and regulators — we make medicines safer for everyone.

Working With Your Medical Team: What Every Patient With Aspergillosis Needs to Know
Modern antifungal treatments, and many of the medicines used alongside them, can be life-saving. They help control infections that would otherwise cause severe damage to the lungs and other organs. But these medicines are also powerful, and like all strong treatments, they sometimes carry risks.
One patient recently shared that they developed nerve damage (neuropathy) while taking antifungal medication, but did not mention it to their doctor because they did not know it could be a side effect. Sadly, problems like this can sometimes become permanent if not spotted early.
This raises an important question: what do patients need to know about their responsibilities when taking medicines like antifungals, and more broadly, when living with aspergillosis?
From passive role to partnership
In the past, healthcare often worked in one direction: the doctor gave instructions, and the patient was expected to follow them. Patients were mostly passive, with little chance to ask questions or take part in decisions.
The NHS is now moving towards a very different way of working: partnership.
This means:
-
Doctors and nurses share their medical knowledge.
-
Patients share their experiences of living with their condition.
-
Together, both sides decide what treatment and care will work best.
Why doctors sometimes hesitate about side effects
Some patients are surprised to learn that not all doctors automatically tell patients about possible side effects. Why is this?
-
Some worry about causing anxiety or putting patients off treatment.
-
Others fear the nocebo effect — where simply knowing about a side effect can make someone more likely to notice it.
-
They may also feel that handing over a long list of possible effects is overwhelming.
But when it comes to antifungals and other long-term, powerful medicines, not knowing can be dangerous. If patients do not know what to look for, they may ignore early signs of serious problems until it is too late.
The best approach is balance:
-
Patients don’t need to memorise an endless list.
-
They do need a clear, short list of the most important and urgent symptoms to look out for — and to know what to do if they appear.
Medicines: what patients should do
-
Take medicines as prescribed – antifungals, inhalers, steroids, or biologics must be taken on schedule. Missing doses can reduce effectiveness or drive resistance.
-
Do not stop suddenly – especially steroids. Always follow tapering advice.
-
Check for interactions – antifungals can clash with common medicines such as statins, blood pressure tablets, and painkillers. Always tell your team about new prescriptions, over-the-counter drugs, or supplements.
-
Use the same pharmacy if possible – so interactions are checked consistently.
Monitoring your health
-
Attend all scheduled tests – blood work, lung function, CT scans. These can reveal hidden changes before you feel them.
-
Know your “normal” – keep track of oxygen levels (if you use a pulse oximeter), peak flow, sputum colour, cough, and breathlessness.
-
Spot infections early – worsening cough, fever, or new sputum colour may mean infection or flare-up. Report these quickly.
Communication with your team
-
Bring notes to clinic – write down questions and symptoms so nothing is forgotten.
-
Be open and honest – if you’ve missed doses, struggled with side effects, or found treatment difficult, let your team know.
-
Keep contact details handy – know who to call if problems arise (specialist nurse, hospital helpline, GP).
Lifestyle and prevention
-
Reduce exposure to moulds – avoid compost heaps, rotting leaves, damp basements, and building dust. If you cannot avoid them, wear an FFP2/3 mask.
-
Protect your lungs – keep up with vaccinations (flu, COVID-19, pneumococcal).
-
Support your overall health – eat well, stay as active as you can, and rest when needed.
-
Look after your mental health – chronic illness is stressful. Patient groups, counselling, or peer support can make a big difference.
Self-management skills
-
Recognise flare-ups – learn the difference between ABPA flare, CPA progression, and bacterial infection symptoms.
-
Know your rescue plan – what to do if you suddenly worsen (extra inhalers, antibiotics, or emergency help).
-
Keep records – note symptoms, hospital visits, and medication changes. This helps spot long-term patterns.
-
Be part of decisions – ask about benefits, risks, and alternatives of treatments. Care should fit your life as well as your lungs.
Where to find reliable information on medicines
Many patients say the leaflet in the medicine box is written in tiny print or feels overwhelming. You do have other options:
-
Ask your clinical team or pharmacist — they can give you a short list of the most important side effects to watch for and explain what’s urgent.
-
Check the BNF (British National Formulary) online — the NHS makes this trusted reference free to the public at bnf.nice.org.uk. It lists side effects, drug:drug interactions, and safety notes.
-
Use NHS.uk — clear pages on most medicines, written in plain English.
-
Patient support organisations — such as the National Aspergillosis Centre or relevant charities, which often provide tailored advice.
If you’re unsure, it’s always safer to ask rather than guess.
The bigger picture: partnership
In the past, doctors made decisions and patients followed instructions. Today, with complex conditions like aspergillosis, patients are central members of the care team.
-
You notice problems first.
-
You take daily responsibility for medication.
-
You decide when to seek help.
This isn’t about shifting the whole burden onto patients — it’s about recognising that care works best when it is a true partnership.
Key message
👉 If you notice something new, strange, or worrying while on antifungal medication — however small — tell your healthcare team. Don’t assume it’s not important.
And remember: safe, effective treatment is a two-way street. Your role as a patient is not just to take medicines, but to observe, record, communicate, and partner with your team. That partnership is what keeps you safe and makes your treatment work.

NHS England - You and Your GP: Key Points for NHS Patients Managing Aspergillosis
You and your general practice (YYGP) has been developed to help patients understand what to expect from their general practice and how they can get the best from their GP team. YYGP also enables patient to provide feedback or raise concerns with their GP Practice, Healthwatch or the integrated care board. The contract requires every GP practice to have linked to the NHS England YYGP document on their website, no later than 1 October 2025.
1. Accessing Your GP
-
Opening hours: Your GP is typically open 8:00 – 18:30, Monday to Friday. You can walk in, call, or use the NHS App or practice website to contact them NHS England.
-
If closed: For urgent but non-emergency needs, use 111 online or by calling 111 NHS England.
-
In an emergency: If symptoms are life-threatening (e.g., sudden severe breathing issues), go to A&E or call 999 NHS England.
2. Making an Appointment
-
When you contact your GP—whether by phone, online, or in person—they’ll assess your condition and respond within one working day with next steps NHS England.
-
This could include:
-
A face-to-face appointment
-
A phone consultation
-
A text message with advice
-
A recommendation to consult a pharmacy or another NHS service NHS England.
-
This prompt response is especially important for aspergillosis fluctuations or side effects from antifungal treatments.
3. Who You'll See
-
You may be seen by a GP, nurse, or pharmacist.
-
If you have a designated carer, they can speak on your behalf (with your permission).
-
If you prefer a specific healthcare professional you trust, request them—though waits might be longer NHS England.
-
Seeing the same clinician regularly can be beneficial for managing complex, long-term conditions like aspergillosis NHS England.
4. Support for Additional Needs
-
If English isn't your first language, you can request interpretation services when booking an appointment.
-
If you need extra help—like longer appointments, a quiet space, wheelchair access, or materials in accessible formats—just let the practice know; they'll try to accommodate NHS England.
5. Changing or Selecting a GP
-
You can find or switch to a GP using the NHS website (“Find a GP”) or by contacting local practices directly NHS England.
-
No ID, NHS number, or proof of address is needed to register—even if you’re homeless or your immigration status is uncertain NHS England.
-
If a practice cannot register you, they must explain their decision in writing within 14 days NHS England.
6. Referral and Treatment Flexibility
-
If your GP refers you to a specialist (e.g., respiratory consultant), you often have the right to choose your hospital or clinic NHS England.
7. Free Care & Private Work
-
GP services are free, including appointments and treatments.
-
Extra services like insurance letters may incur a fee NHS England.
8. Being a Helpful Patient
-
Prepare for appointments: list symptoms, treatment concerns, and questions in advance.
-
Be punctual or cancel in good time to avoid delays for others.
-
Use the NHS App or website to book appointments, refill prescriptions, and view test results.
-
Turn on App notifications to stay updated with messages from your practice NHS England.
-
Order repeat prescriptions well ahead—especially vital when managing antifungal medications—to avoid running out NHS England.
-
Consider joining the Patient Participation Group at your practice to share feedback and help improve services NHS England.
9. Sharing Feedback or Concerns
-
To raise concerns, talk to your practice manager first.
-
If needed, you can escalate feedback to your local Integrated Care Board (ICB).
-
You can also reach out to your local Healthwatch (an independent NHS watchdog) for confidential advice and support NHS England.
Why This Matters for Aspergillosis Patients
Aspergillosis often requires ongoing monitoring, regular breathing tests, imaging, and antifungal therapy adjustments. Timely access to GP services, continuity of care, and preparedness all enhance your ability to manage flare-ups or side effects effectively.
Handy Checklist (for easy reference)
| Task |
|---|
| Contact GP promptly for new or worsening symptoms |
| Prepare questions ahead—e.g., changes in breathing, treatment effects |
| Use NHS App to manage appointments and medications |
| Order repeat prescriptions early to maintain drug access |
| Request support services if needed (interpretation, accessibility) |
| Provide feedback to improve your experience and others' |

Shared Care Records in the NHS: What Aspergillosis Patients Need to Know
The NHS is changing how patient records are managed. By 2026, every area of England will have a Shared Care Record. This is not one big “national record,” but a way of securely linking together the different records held by your GP, hospital, and other services.
For patients with aspergillosis, this could make a real difference to care, safety, and research.
🗂 What Is a Shared Care Record?
-
Not one single file: Your GP, hospital, and community services keep their own systems.
-
Linked together: Clinicians can securely view a joined-up picture of your health.
-
Safer and faster care: Your allergies, test results, and medications can be seen wherever you are treated.
-
You tell your story once: No more repeating details every time you see a new doctor.
🛡 How Safe Is My Data?
-
Strict access control: Only staff directly involved in your care can open your record.
-
Audit trail: Every time it’s viewed, the system records who, when, and why.
-
Encryption & firewalls: Records are locked against outside access.
-
No mass downloads: Systems only allow one patient’s record at a time.
In many ways, this is safer than old paper notes, which could be lost, copied, or seen by accident.
👩⚕️ Confidentiality Rules Stay the Same
-
NHS staff are bound by confidentiality laws and the Caldicott Principles.
-
Looking at a record without a valid care reason is a disciplinary offence.
-
Your record is not shared with insurers, employers, or relatives without your consent.
📊 Research and Aspergillosis
Shared Care Records could also help improve research into aspergillosis, which is often under-recognised:
-
Better case finding: Linking GP, hospital, and lab data makes it easier to identify true cases.
-
Tracking outcomes: Researchers can follow IgE/IgG results, CT changes, and treatment responses over time.
-
Environmental links: Data could be combined with housing, air quality, and weather information.
-
Support for trials: Easier to find eligible patients for new antifungal or biologic studies.
All research use is usually de-identified (your name and personal details removed). You can choose to opt out via the National Data Opt-Out if you don’t want your data used in this way.
🏦 Will Insurance Companies See My Record?
No. Insurance companies and employers cannot access your NHS record.
If you apply for insurance, your GP may be asked for a report — but this is only done with your consent.
🌐 What If I Don’t Use the Internet?
You don’t need to be online to benefit. Shared Care Records are mainly for clinicians, not for patients logging in.
If you want to see your record, you can still ask for a paper copy from your GP or hospital.
📍 Who Runs Shared Care Records?
They are organised locally by Integrated Care Systems (ICSs).
-
England is divided into 42 ICSs, each bringing together NHS services, local councils, and community care.
-
Examples include Greater Manchester ICS, Cheshire & Merseyside ICS, and North East London ICS.
-
Scotland, Wales, and Northern Ireland use different systems.
✅ Key Reassurances for Patients with Aspergillosis
-
Your data remains confidential and secure.
-
Shared Care Records mean joined-up, safer care across GP, hospital, and community services.
-
Insurers and employers cannot access your NHS record.
-
You stay in control — you can opt out of data use for research if you wish.
-
The new system could help advance aspergillosis research, leading to better diagnosis and treatments.
🩺 NHS Data Sharing: How It Will Improve Your Care
🌍 The Problem Today
At the moment, your health information is stored in many different places:
-
Your GP (General Practitioner) has one record.
-
Hospitals keep their own records.
-
Community services (like district nurses or physiotherapists) have separate notes.
-
Social care also keeps its own information.
This can cause problems:
-
You may be asked to repeat your story again and again.
-
Doctors don’t always see the full picture (medications, allergies, past test results).
-
Sometimes tests are repeated unnecessarily.
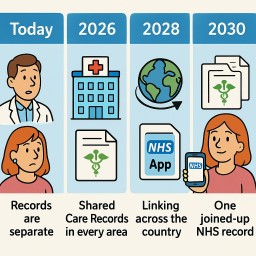
📅 The Timeline for Change
Today (2025)
-
Records are mostly separate.
-
Some areas already share basic information like your medicines and allergies through a “Summary Care Record.”
👉 What it means for you: You still have to repeat information at most appointments.
2026 – Shared Care Records in Every Area
-
Every region (called an Integrated Care System, or ICS) will have a Shared Care Record.
-
This links together information from GPs, hospitals, community teams, and social care.
-
Hospitals using modern systems like Epic (a type of electronic patient record - MFT has installed this already) can also start sharing directly with other Epic hospitals.
👉 What it means for you: Doctors can see more of your health record without asking you to repeat everything.
2028 – Linking Across the Country
-
Regional Shared Care Records will start to connect with each other.
-
Epic hospitals across the UK will share records more easily using Care Everywhere (Epic’s sharing tool).
-
Community services and “virtual wards” (hospital care at home) will be fully connected.
👉 What it means for you: If you are treated in another part of the country, staff there will be able to see important parts of your health record straight away.
2030 – One Joined-Up NHS Record
-
The NHS plans to give every patient a longitudinal record – one joined-up health and care record that follows you everywhere.
-
This will combine information from GPs, hospitals, community services, mental health teams, and social care.
-
Patients will also be able to see much more of their own record through the NHS App.
👉 What it means for you: Wherever you go in the NHS, staff can see your medical history safely. You’ll feel your care is joined-up, and you can also check your record yourself.
✅ Your Patient Journey: Step by Step
-
Today: “I have to explain my medication list every time. I’m not sure my hospital knows what my GP prescribed.”
-
2026: “When I go into hospital, the doctor can already see my GP record and community nurse notes.”
-
2028: “I was treated far from home, and the hospital could see my recent test results straight away.”
-
2030: “Wherever I go, the NHS staff have the full picture. I can see my record too on the NHS App.”
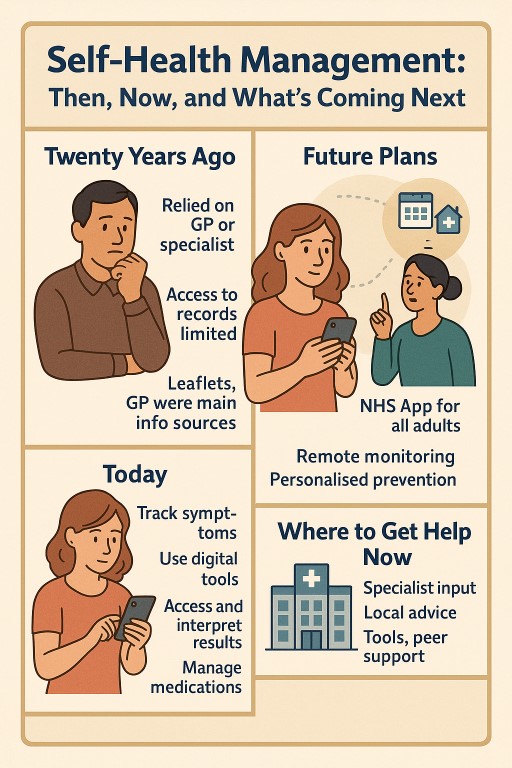
🧭 Self-Health Management: Then, Now, and What’s Coming Next
🧭 Self-Health Management: Then, Now, and What’s Coming Next
Over the past 20 years, the way people manage their health in the UK has changed dramatically — and more changes are on the horizon. For people living with long-term or complex conditions like aspergillosis, asthma, or chronic lung disease, this shift has brought both new opportunities and new burdens.
This article explains what’s changed, what the government is planning, what benefits are hoped for — and what happens if you can’t or don’t want to use online tools.
🕰️ What Was Self-Health Management Like 20 Years Ago?
In the early 2000s:
-
Patients relied heavily on their GP or hospital specialist for every decision.
-
Access to records was limited or non-existent.
-
Health information came from leaflets, GPs, or occasional TV programmes.
-
Appointments were mostly face-to-face and arranged by phone.
-
There was less expectation for people to self-manage complex conditions.
📲 What’s Different Today?
Patients today are expected to:
-
Track symptoms themselves and know when to seek help.
-
Use digital tools like the NHS App, online consultations, and health monitoring apps.
-
Interpret test results, medication side effects, and care plans with less direct support.
-
Coordinate care between services — sometimes across different hospitals or systems.
-
Understand and act on complex health advice, often with less contact from clinicians.
For people with chronic respiratory conditions like CPA or ABPA, this can sometimes improve control — but it can also feel overwhelming, especially when care is fragmented or specialists are hard to reach.
🧑⚕️ How Are Healthcare Staff Adapting?
Many GPs, nurses, and hospital teams are trying to:
-
Embrace shared decision-making and educate patients more directly.
-
Offer video, phone, or online consultations when appropriate.
-
Provide tools like self-monitoring diaries, peak flow meters, or oxygen saturation monitors.
-
Rely on electronic triage systems and limit in-person appointments to the most complex cases.
But many are also under pressure. Staff shortages, long waiting lists, and increased demand mean clinicians have less time per patient, making it harder to offer the detailed guidance many people still need.
🏛️ What Is the UK Government Planning for the Future?
The government’s current plans aim to make the NHS more digital, preventative, and self-directed. This is laid out in the NHS Long Term Plan, the Digital Health and Care Strategy, and the Data Saves Lives policy.
| Goal | Target |
|---|---|
| Make the NHS App the main access point for care | 2025–2026 |
| Move more routine care to remote monitoring and self-management | By 2026–2029 |
| Personalise prevention and reduce avoidable illness | By 2029 |
| Reduce reliance on face-to-face appointments | Ongoing since 2021 |
| Digitise health records across all services | By 2025–2027 |
Patients with long-term conditions are expected to:
-
Manage their own prescriptions
-
Monitor symptoms at home
-
Use digital tools to stay informed and in control
-
Access care only when needed, rather than by default
🎯 What Are the Hoped-For Benefits?
The government promotes these changes as delivering:
✅ Better Outcomes
-
Early intervention, better symptom tracking, and fewer complications.
-
Personalised care plans based on your data and condition.
✅ More Convenient Care
-
Fewer unnecessary visits
-
More control over your own information and appointments
✅ NHS Cost Savings
-
Reducing face-to-face appointments and hospital stays frees up staff time.
-
Less duplication, fewer unnecessary tests, better resource use.
⚠️ But Is It Better for Everyone?
Not necessarily. These benefits are not equally felt by all patients.
🧓 Digital Exclusion Is a Real Problem
-
Around 1 in 5 UK adults struggle with using digital health services.
-
Older adults, people on low incomes, and those with disabilities or learning needs are most affected.
-
Some patients simply don’t feel confident, or don’t trust digital systems.
🧭 What Happens If You’re Left Behind?
Government guidance insists that non-digital options must remain — but this isn’t always consistent. Some patients report:
-
Difficulty reaching practices by phone
-
Online-only booking or consultations
-
Fewer letters and face-to-face reviews
Patients with complex, fluctuating, or rare conditions like aspergillosis may find it harder to get appropriate support without a strong digital presence — especially if care crosses multiple departments or regions.
🧠 So What Needs to Happen?
To make this shift work for everyone, the system must:
-
Protect non-digital access routes (e.g. phone, letter, face-to-face)
-
Offer digital training and support to those who want it
-
Make sure apps and online tools are inclusive and easy to use
-
Involve patients in designing these services — especially those with long-term conditions
-
Keep monitoring for harm or exclusion, and respond quickly
📍 Where Can Patients Get Help Today?
| Support Type | Where to Find It |
|---|---|
| 🔬 Specialist advice | National Aspergillosis Centre, hospital respiratory clinics |
| 👨⚕️ Local support | GP, pharmacist, practice nurse |
| 📱 Digital tools | NHS App, condition-specific apps, NHS websites |
| 🤝 Peer support | Online groups, charities, forums (e.g. Asthma + Lung UK, aspergillosis.org) |
| 💬 Advice lines | NHS 111, condition-specific helplines |
✅ In Summary
The NHS is changing — and patients are expected to change with it. Over 20 years, self-management has gone from optional to expected, and digital care is being rapidly expanded.
For some, this means more control and quicker help. For others, it can feel isolating, confusing, or unsafe. The challenge is to design systems that support everyone — not just the tech-savvy or well-connected.
If you’re living with a long-term condition like aspergillosis, you should never be left managing alone.

🧾 Getting a Second Opinion for Aspergillosis: What If Your Hospital Refuses?
Many patients living with aspergillosis or allergic bronchopulmonary aspergillosis (ABPA) ask for a second opinion — often from a national centre like the National Aspergillosis Centre (NAC) in Manchester or from another specialist elsewhere in the UK. But sometimes, hospitals resist sending your case outside their own department.
Here’s what’s happening, why it might occur, and what you can do.
🤔 Why Would a Hospital Refuse an Outside Opinion?
It’s understandably frustrating when you’ve asked for expert help and your local hospital insists on keeping things “in-house.” Here are some reasons this might happen:
1. Internal Referral Rules
Hospitals sometimes have a policy to refer to another consultant within their own department first. They may consider this a “second opinion,” even if it’s not truly independent.
2. Cost and Complexity
Referrals to another NHS trust — especially across health boards or into England (e.g. to NAC) — can involve extra steps and costs. Some hospitals prefer to avoid that unless they feel there’s no choice.
3. Professional Sensitivities
Some doctors may feel a national second opinion implies criticism of their care, even if your request is made respectfully.
4. Lack of Awareness
Some clinicians aren’t fully aware of what the National Aspergillosis Centre offers — or may underestimate how complex aspergillosis, ABPA, or recurrent fungal infections can be.
🧑⚕️ But Isn’t a Specialist Opinion My Right as an NHS Patient?
Yes. If your GP or hospital team believes it’s clinically appropriate, you have the right to be referred to another NHS consultant — including one outside your local area.
The NAC is nationally commissioned by NHS England to provide care for people with chronic aspergillosis. They accept referrals from across the UK.
💷 Why Private Care Might Not Be an Option
Some patients consider going private when local NHS referrals are blocked — but private care often means:
-
Paying for new scans, blood tests, and sputum cultures
-
No direct access to previous NHS records
-
Higher costs than expected, especially for complex tests
If you can’t afford this, you are not alone, and there are still NHS options available.
🧭 What You Can Do Next
Here are practical steps if you're being blocked from getting a second opinion:
✅ 1. Restate Your Request Clearly
Ask your GP (or write yourself) to reply to the hospital and explain:
-
You are specifically asking for an opinion from a national expert service (e.g. NAC or Dr Iain Page in Edinburgh).
-
This is not a rejection of their care, but a request for specialist reassurance, diagnosis support, or treatment planning.
✅ 2. Ask for a Tertiary Centre Referral
Use the term “tertiary referral” — this means a referral to a national or highly specialised NHS service.
✅ 3. Raise It with PALS
If you're still being blocked, contact your local Patient Advice and Liaison Service (PALS) or NHS complaints team. Explain:
-
You have a rare/complex condition,
-
You’ve asked for a national review,
-
And you’ve been offered only an internal opinion.
✅ 4. Get support on NAC Support Facebook Group
- https://www.facebook.com/groups/aspergillussupport/
💬 In Summary
-
You’re not being difficult — you’re advocating for your health.
-
It is reasonable and often necessary to seek input from specialists like those at the NAC.
-
If you’ve been told “no,” it may be due to policies or misunderstandings — not a reflection on your need for better care.
-
Keep asking, and if needed, involve your GP, or PALS.
Key Shifts to Reinvent the NHS - The 10 Year plan
The plan introduces three radical shifts to modernize the NHS and secure its future:
-
🏥 Hospital → Community
-
Build a Neighbourhood Health Service: community health centres open 6 days/week for 12 hours/day
-
Provide integrated care closer to home—GPs, diagnostics, mental health, rehab, dentists, pharmacists, and even social support
-
Aim to reduce reliance on hospitals and cut waiting lists
-
-
📱 Analogue → Digital
-
Transform the NHS App into a “doctor in your pocket”—for appointments, advice, care plans, and self-referral
-
Embed AI to reduce admin, transcribe consultations, and support clinical decision-making
-
-
🛡️ Sickness → Prevention
-
Emphasize early intervention through more health checks, screenings, vaccines, and public health services
-
Shift funding towards community and preventative care, away from reactive hospital-based services
-
🏗 Underpinning Measures
To support these shifts, the plan introduces:
-
A new operating model & statutory framework to streamline the NHS structure
-
Transparency and accountability through metrics and patient feedback
-
Workforce transformation, including new training and wellbeing support
-
Innovation strategy harnessing genomics, AI, and tech
-
Financial reform via value-based funding—where providers are rewarded for outcomes
🔍 What This Means for You
-
Access to GP advice and care should be faster and more local – with reduced “8 am scramble”
-
More services like scans, mental healthcare, rehab, smoking cessation, and job support delivered at local centres
-
Greater convenience—use the App to manage care, book appointments, or message clinicians
-
Stronger focus on staying healthy—through screening, prevention, and early treatment support
🧩 Challenges & Expert Views
-
Funding & staffing: A £29 billion investment is pledged, but staffing shortages and infrastructure needs remain concerns
-
Implementation: Organisations like the King’s Fund highlight the absence of operational details and worry pilot projects may lead to regional variation
-
Behavioural shift: Success depends on NHS culture evolving—from reactive treatment to proactive, tech-enabled care
✍️ Final Take
The 10‑Year Health Plan represents a transformative vision: bring care closer to home, empower patients digitally, and focus on prevention. With strong backing from Starmer and Health Secretary Streeting, it aims to reshape NHS services by 2035. While optimism is growing, the effectiveness of implementation and securing resources will determine whether it truly delivers for patients and staff.

From Cradle to Shared Care: Understanding the NHS Transition to Patient Partnership
The NHS is evolving. From its early days as a post-war health service built around face-to-face care by a GP who "did it all," to today’s complex model focused on prevention, digital access, and patient partnership — the change has been profound. This document provides a clear overview of why, how, and where the NHS is transitioning toward shared care and self-management.
📜 Then and Now: The 1960s NHS vs Today
The NHS in the 1960s:
- Care was largely reactive — you went to the doctor when you were ill.
- GPs were central and often lifelong figures in a family’s care.
- Most treatments were limited, and few people lived long with chronic illness.
The NHS Today:
- Patients live longer, often with multiple long-term conditions.
- Care must be proactive and coordinated.
- The NHS encourages patients to understand and manage their health.
- The model is increasingly digital, multidisciplinary, and patient-centred.
⚙️ Why the Shift Happened
- Rising Chronic Illness: Diabetes, heart disease, asthma, and mental health issues have all increased.
- Ageing Population: More people need long-term support.
- Advances in Medicine: Enable people to live longer but require more daily self-care.
- Resource Constraints: GP and hospital services are under increasing pressure.
- Better Outcomes with Patient Involvement: Evidence shows shared care leads to better results.
📈 Timeline of Change
| Year | Event |
|---|---|
| 2008–2010 | Expert Patient Programmes piloted |
| 2014 | Five Year Forward View introduces prevention and self-care |
| 2019 | 🚀 NHS Long Term Plan launches personalised care model |
| 2020 | Universal Personalised Care policy published |
| 2021–2022 | COVID accelerates digital triage and remote monitoring |
| 2023–2025 | Integrated Care Systems tasked with delivering shared care |
| 2025 | 📣 Anticipated release of the next major NHS reform report by the current government, expected to include a 10-year plan focusing on community-based care, digital access, and integration with social care |
🧠 What Is Shared Care?
Shared care is a model where:
- Patients are active partners, not passive recipients.
- GPs, nurses, pharmacists, and support workers form a care team.
- People with long-term conditions have personalised care plans.
- Patients are supported to self-monitor and make informed decisions.
📊 Evidence of Impact
- Diabetes & Hypertension: Better control when patients co-manage.
- Asthma & COPD: Action plans reduce flare-ups and hospital visits.
- Mental Health: Shared decision-making improves engagement and outcomes.
- BMJ & Cochrane Reviews: Shared care reduces hospital use and improves satisfaction.
👥 What About Those Without Digital Access?
Digital exclusion affects:
- Older adults
- People with learning difficulties or low literacy
- People without smartphones or broadband
Solutions:
- Maintain paper and telephone options
- Offer face-to-face access when needed
- Train staff to identify and support non-digital patients
- Invest in community digital skills projects
⏳ How Far Along Are We?
We’re mid-transition:
- Policy is in place across England.
- ICSs are developing care coordination teams.
- Self-monitoring and digital records are expanding.
- But delivery is uneven, and many staff need more support and training.
Estimated full embedding of shared care: 2028–2032, depending on region and resources.
🩺 Does the NHS Still Care for Us from Cradle to Grave?
Yes — but with an evolved model:
- Still free at the point of care
- Still lifelong
- But now expects patients to:
- Learn about their condition
- Monitor their health
- Use digital or alternative access routes
- Take shared responsibility for staying well
The shift is from "We’ll do it for you" → to "We’ll support you to do it together."
🏥 The Role of Private Healthcare in the Shared Care Era
Private care plays a growing role alongside the NHS, especially where speed, access, or choice is limited:
Where it helps:
- Faster diagnosis or specialist review
- Choice of clinician and continuity
- Access to treatments not available on the NHS
- Supplementary services like physio or counselling
Limitations:
- Not all can afford it — risk of health inequality
- Poor integration with NHS records
- Standards vary between providers
In context: Private care can complement the NHS, especially for people managing long-term conditions, but it should never replace inclusive, high-quality NHS care. Patients benefit most when systems are coordinated, and no one is left behind.
💷 Will Shared Care Make the NHS and Social Care Cheaper?
In theory, yes — but in practice, it’s more complicated. Shared care and self-management are designed not just to improve health outcomes, but also to reduce long-term demand on overstretched NHS and social care services.
📉 Potential Savings
| Area | How Shared Care Could Save Costs |
| Hospital admissions | Fewer A&E visits and unplanned admissions (e.g. asthma, heart failure) |
| GP appointments | More issues resolved by nurses, pharmacists, or self-care tools |
| Social care needs | Better-managed health can delay or reduce dependency on care packages |
| Medication | Improved adherence and fewer avoidable prescriptions or interactions |
| Workforce efficiency | Tasks redistributed to broader care teams (e.g. care coordinators, link workers) |
⚠️ Upfront Costs to Consider
- Training staff in personalised care and shared decision-making
- Investing in digital systems and patient tools
- Supporting digitally excluded or vulnerable groups
- Funding community-based roles (link workers, social prescribers)
🧮 What the Evidence Says
- The Health Foundation (2021) found that shared care is often cost-effective but savings take years to appear.
- Diabetes Prevention Programmes and home blood pressure monitoring schemes have demonstrated long-term cost reductions when patients are well supported.
- ICSs are beginning to measure value not just in pounds saved, but in avoidable harm and hospital use prevented.
Shared care isn’t a quick fix for NHS finances — it’s an investment in long-term sustainability.
🔗 Do We Need a More Fully Integrated NHS and Social Care?
Yes — integration is essential if shared care is to work effectively.
Currently, NHS healthcare and local authority social care operate through separate budgets, systems, and eligibility rules, which can lead to gaps, delays, or duplication. For patients with complex needs — such as older adults, people with disabilities, or those with long-term conditions — this separation often causes frustration and poorer outcomes.
Why Integration Matters:
- 🧓 Smooth transitions from hospital to home
- 📋 Unified care plans that cover medical, practical, and emotional support
- 🤝 Fewer assessments and handoffs between services
- 💡 Faster responses when needs change
What’s Already Happening:
- Integrated Care Systems (ICSs) aim to bring NHS and social care leaders together
- Some areas are piloting pooled budgets or joint appointments
- Shared care records are being rolled out in regions to link GP, hospital, and social services
Barriers to Integration:
- Separate funding structures (NHS = national, Social Care = local authority)
- Different eligibility rules and charging systems
- Workforce shortages and incompatible IT systems
True shared care requires shared systems, shared responsibility — and shared investment.
🧭 What Support Exists to Help Patients Transition to Shared Care?
As the NHS shifts toward shared care and patient partnership, new support services and resources have been introduced to help patients take on a more active role in their health.
🧑⚕️ Where Patients Can Get Help:
- GP Practices: Many now have a wider team including:
- Care coordinators
- Health and wellbeing coaches
- Social prescribers
- Practice nurses trained in personalised care
- Pharmacies: Community pharmacists can support minor illnesses, medication reviews, and some chronic condition monitoring.
- The NHS App: Allows patients to:
- View medical records
- Order prescriptions
- Access care plans and vaccination status
- Link to symptom checkers and self-care tools
- Patient Support Groups and Charities: Many long-term condition charities (e.g. Asthma + Lung UK, Diabetes UK, Versus Arthritis) offer:
- Peer support
- Online education
- Print resources
- Helplines
- Community Services (varies by area):
- Self-management education courses (e.g. Expert Patients Programme)
- Voluntary sector health coaches or befriending schemes
- Local authority or ICS-run wellbeing hubs
📞 If in Doubt, Ask:
- Contact your GP reception and ask: “Can I speak to someone about managing my condition better?”
- Many areas have health navigators who can connect you to appropriate services.
The transition is not just about expectations — it comes with real support. No one should be left to do it alone.
🎯 Final Thought
The NHS of today — and tomorrow — is built around partnership. While some miss the simplicity of the old model, the future offers tools and support that can help people live longer, healthier lives — if everyone is included. Shared care works best when:
- Patients feel supported
- Clinicians feel equipped
- Services stay flexible and inclusive
🫁 Why Is CPA Called a Long-Term Condition — Not a Lifelong One?

Chronic Pulmonary Aspergillosis (CPA) is often described as a long-term condition, but people sometimes wonder why it isn’t called a “lifelong” disease — especially since many people need antifungal treatment and regular monitoring for years.
Here’s what we know:
🩺 CPA Affects Everyone Differently
CPA is a complex condition that includes several forms — some people have a single fungal ball (aspergilloma), while others have more widespread or progressive disease. For many, CPA needs long-term treatment, such as antifungal tablets, oxygen, physiotherapy, or hospital care.
But not everyone has the same experience:
-
Some people are stable for years
-
Some respond well to treatment and no longer need antifungals
-
Others may live with occasional flare-ups or long-term health problems
🔁 Why It’s Not Always Called Lifelong
CPA is called a “long-term condition” because:
-
It typically lasts at least a year, often longer
-
It may come and go in phases
-
It needs regular follow-up and may affect daily life
But not everyone will have it for the rest of their life — and that’s why we don’t use the word “lifelong” for everyone.
🔬 We Don’t Yet Know Who is Truly ‘Cured’
To say whether CPA is curable, we would need to:
-
Follow a large group of patients
-
For many decades
-
To see who stays well and never relapses
That kind of long-term research is still ongoing — so at the moment, doctors can’t say for sure when or if someone is permanently cured.
Some people stay well for years after stopping treatment — but it’s too early to know if the infection is truly gone, or just sleeping.
💬 What This Means for You
-
CPA is a condition that can be managed — sometimes very successfully
-
You might not need treatment forever — but regular check-ups help catch any changes early
-
Your team will work with you to find the right balance of treatment and independence
-
If you feel well, that's a good sign — but it's still important to keep an eye on things
📍In short: CPA is a serious, long-term condition, but it’s not always lifelong. We still have more to learn, and long-term studies are helping us understand it better every year.