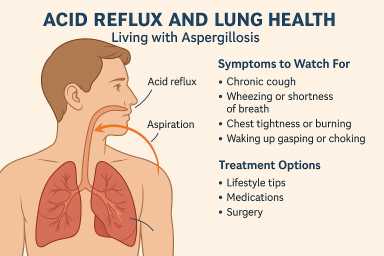
Living with Aspergillosis

📁 Coping with Steroid Side Effects and Finding Balance: A Guide for Aspergillosis Patients
Living with chronic forms of…

🌿 Living Well with Aspergillosis: Understanding the Role of Palliative Care
Many people think palliative…
🌫️ A Life Shaped by Mould: One Person’s Journey with CPA and Lung Disease
Sadly, at the time of writing…


