We usually think of winter as…
by Beth Bradshaw
by GAtherton
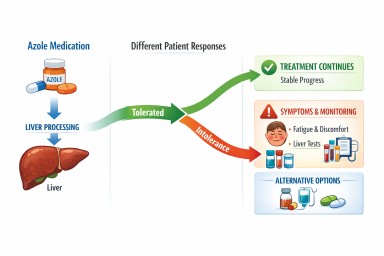
Last reviewed: April 2026…
You are not alone with…
Last reviewed: 18 March 2026…
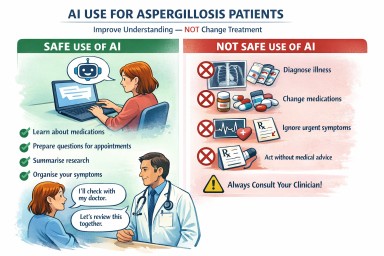
Artificial intelligence (AI)…
Home › Knowledge Hub ›…
A supportive message for…
A practical, evidence-based…