CPA
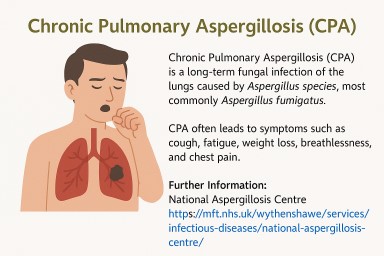
⭐ Chronic Pulmonary Aspergillosis: Why Diagnosis Is Missed and Who Needs to Be More Aware
With estimated prevalence of…


🌬️ Inhaled Antifungal Treatments for Chronic Pulmonary Aspergillosis (CPA)
Updated: October 2025 💡 Why…


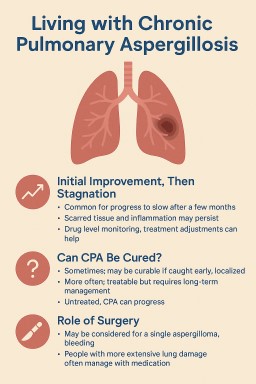
🌫️ A Life Shaped by Mould: One Person’s Journey with CPA and Lung Disease
Sadly, at the time of writing…