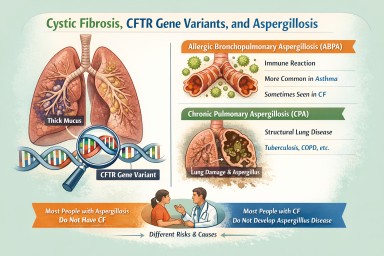
CPA


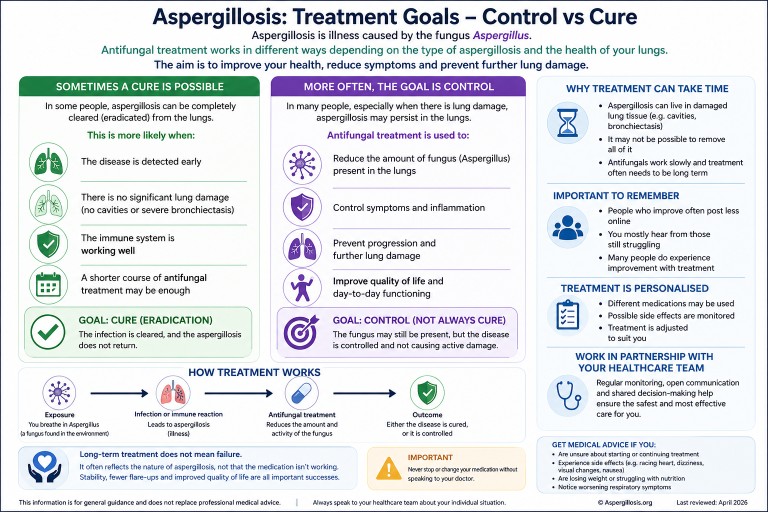
Can Aspergillosis Be Cured? Understanding Treatment, Control, and Long-Term Therapy
Last reviewed: April 2026…
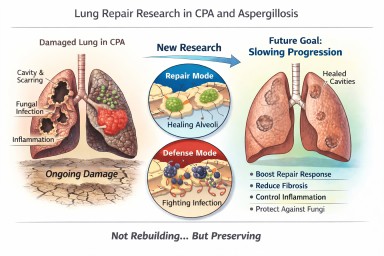
Looking further into the future - could we control lung damage, preserve healthy lung tissue better?
Can Lungs Repair Themselves?…

Can blood tests help predict if chronic pulmonary aspergillosis will come back?
This study from the National…