Aspergillus Bronchitis

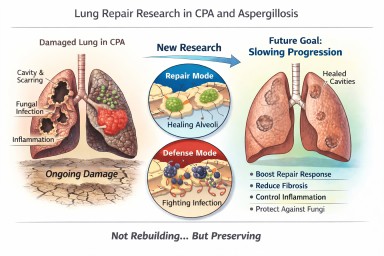
Looking further into the future - could we control lung damage, preserve healthy lung tissue better?
Can Lungs Repair Themselves?…
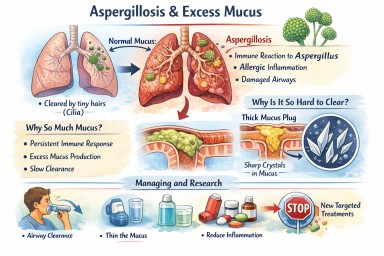

⭐ Aspergillus Bronchitis: The Overlooked Condition Hiding in Plain Sight
Estimated prevalence 1–2% in…
