Looking further into the future - could we control lung damage, preserve healthy lung tissue better?
Can Lungs Repair Themselves?
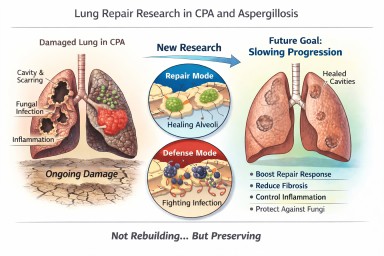
What New Research Means for People with CPA (and Other Aspergillosis)
A recent scientific discovery has helped researchers understand how certain lung cells decide whether to focus on repairing damage or defending against infection. The work, highlighted by the Mayo Clinic and published in Nature Communications, describes a molecular “switch” inside specialised lung cells that influences this balance.
For people living with Chronic Pulmonary Aspergillosis (CPA) — and also those with Allergic Bronchopulmonary Aspergillosis (ABPA) — this kind of research is relevant. But it needs careful explanation.
This is not about rebuilding destroyed lungs.
It is about understanding how to better protect and preserve the lung tissue that remains.
The Discovery: A “Repair vs Defence” Switch
Researchers identified a regulatory circuit in alveolar type II (AT2) cells — specialised cells that:
-
Produce surfactant (which keeps air sacs open)
-
Act as a reserve “repair” population in the lung
-
Can regenerate other essential lung cells after injury
The study showed that these cells operate under tight control. When infection is present, they prioritise defence. When injury needs healing, they can switch into repair mode.
The key insight is that this switch is biologically regulated. It is not random. That means, in theory, it may one day be possible to influence it.
What “Repair” Means — and What It Does Not Mean
When we talk about lung repair in this context, we must be very clear.
It does not mean:
-
Lung cavities caused by CPA will close in the foreseeable future
-
Established fibrosis will melt away
-
Bronchiectasis will reverse
-
Severely distorted lung architecture will rebuild
CPA cavities represent major structural remodelling — destruction of alveoli, scarring, altered blood supply, and thickened pleura. Reconstructing that complex architecture is biologically extremely challenging and not currently realistic within the next decade.
What repair does realistically mean
In chronic lung disease, “repair” is more likely to mean:
-
Supporting survival of remaining alveoli
-
Preventing excessive fibrotic signalling
-
Helping lung lining cells recover more efficiently after inflammation
-
Reducing cumulative injury from repeated infection
-
Slowing progression of structural change
In other words:
Not rebuilding what is gone — but better protecting what remains.
For many people with CPA, this is a crucial distinction.
Why Preservation Is a Major Goal in CPA
CPA usually develops in lungs already weakened by conditions such as tuberculosis, non-tuberculous mycobacteria, chronic obstructive pulmonary disease, or severe pneumonia.
Over time, CPA can lead to:
-
Expanding cavities
-
Progressive scarring
-
Reduced gas exchange
-
Reduced exercise tolerance
Many patients have limited lung reserve. Even small additional losses of functioning lung tissue can significantly increase breathlessness or fatigue.
If future therapies could slow the rate of progression — even modestly — that would meaningfully affect long-term outcomes.
Flattening the decline curve is not trivial. It changes quality of life.
Why This Also Matters in ABPA
In ABPA, repeated inflammatory episodes can lead to:
-
Airway remodelling
-
Mucus plugging
-
Development or progression of bronchiectasis
Better control of inflammatory signalling — combined with improved epithelial recovery — could reduce long-term airway damage.
Again, this is about preservation rather than reversal.
Where Development Has Reached
The current research is still laboratory-based. It used advanced techniques such as:
-
Single-cell sequencing
-
Imaging of lung tissue
-
Preclinical models of injury
No human treatments based on this discovery are yet available.
However, the significance lies in identifying:
-
A defined molecular pathway
-
A controllable regulatory mechanism
-
A clearer understanding of why repair fails in chronic inflammation
That foundational knowledge is what eventually allows targeted drug development.
The Balance Challenge in Aspergillosis
There is an additional complexity in fungal lung disease.
Any attempt to promote repair must not weaken antifungal defence.
The immune system must:
-
Control Aspergillus
-
Avoid causing excessive inflammatory damage
Future therapies would need to strike that balance carefully.
What This Means for Patients Now
This discovery does not change current treatment.
The most effective preservation strategies today remain:
-
Consistent antifungal therapy when indicated
-
Careful inflammatory control
-
Biologic therapies where appropriate
-
Airway clearance
-
Vaccination and infection prevention
-
Avoiding damp and mould exposure
-
Pulmonary rehabilitation
These measures are already forms of lung preservation.
A Realistic and Hopeful Perspective
It is unlikely that cavities from CPA will be repaired in the near future.
It is realistic that within the next 5–10 years we may see improved strategies aimed at:
-
Slowing structural progression
-
Supporting endogenous repair cells
-
Reducing fibrotic signalling
-
Improving recovery after exacerbations
For people living long-term with CPA or ABPA, even incremental preservation could significantly affect independence and quality of life.
The science is still early — but understanding how the lung decides to repair itself is an important step forward.
Reference
Sawhney, A.S., Deskin, B.J., Cai, J. et al. A molecular circuit regulates fate plasticity in emerging and adult AT2 cells. Nat Commun 16, 8924 (2025). https://doi.org/10.1038/s41467-025-64224-1