For people with Allergic Bronchopulmonary Aspergillosis (ABPA), severe asthma and other forms of aspergillosis, steroid treatment can be both extremely helpful and medically complicated.
Many patients are prescribed corticosteroids such as prednisolone or methylprednisolone to control inflammation, improve breathing and reduce the risk of lung damage. These medicines can be very effective. However, repeated or long-term steroid treatment can also affect the body’s natural hormone system, especially the adrenal glands.
Some patients are told:
- “Your cortisol is low.”
- “Your ACTH level is abnormal.”
- “You may have adrenal suppression.”
- “This may be steroid withdrawal.”
- “The blood tests are difficult to interpret.”
This can be worrying and confusing, especially when symptoms are severe but the explanation is not straightforward.
This article explains why adrenal problems can occur in some people with aspergillosis and severe asthma, why blood tests such as cortisol and ACTH can be difficult to interpret, and why steroid treatment sometimes involves a careful balance between benefit and risk.
Key points summary
- Steroid medicines can reduce the body’s own natural cortisol production.
- This is called adrenal suppression or adrenal insufficiency.
- Symptoms may overlap with aspergillosis, asthma, infection, fatigue or steroid withdrawal.
- Blood tests such as cortisol and ACTH can be difficult to interpret.
- Inhaled steroids and antifungal medicines can also influence steroid effects.
- Long-term prednisolone is generally avoided where possible, but it may still be necessary for some patients.
- Patients should not stop or reduce steroids suddenly without medical advice.
- Severe symptoms such as collapse, vomiting, dehydration, confusion or severe weakness require urgent medical advice.
Contents
- What do the adrenal glands do?
- What are cortisol and ACTH?
- Why are steroids used in ABPA and aspergillosis?
- Are steroids only meant for short-term use?
- How steroids affect the body’s natural hormone system
- What is adrenal suppression?
- Why symptoms can be difficult to recognise
- Why blood tests can become confusing
- The role of inhaled steroids
- Antifungal medicines and steroid interactions
- Steroid withdrawal versus adrenal insufficiency
- What kinds of stress may require higher steroid doses?
- When should patients seek urgent medical advice?
- Frequently asked questions
- Final thoughts
What do the adrenal glands do?
The adrenal glands are small glands that sit above the kidneys. They produce several important hormones, including cortisol.
Cortisol helps the body:
- respond to stress,
- maintain blood pressure,
- regulate energy levels,
- support immune function,
- and cope with illness or infection.
The body carefully controls cortisol levels through a hormone signalling system involving the brain, the pituitary gland and the adrenal glands.
What are cortisol and ACTH?
ACTH stands for adrenocorticotropic hormone.
The pituitary gland in the brain releases ACTH to tell the adrenal glands to produce cortisol.
This system normally works as a feedback loop:
- When cortisol is low, ACTH usually rises.
- When cortisol is high, ACTH usually falls.
Cortisol levels naturally change during the day and are usually highest in the early morning. This is one reason why many cortisol blood tests are taken around 9am.
Why are steroids used in ABPA and aspergillosis?
In Allergic Bronchopulmonary Aspergillosis (ABPA) and some severe asthma conditions, the immune system reacts strongly to Aspergillus fungi.
This can cause:
- airway inflammation,
- wheezing,
- coughing,
- mucus plugging,
- breathlessness,
- worsening lung function,
- and repeated flare-ups.
Steroids such as prednisolone are often used because they reduce inflammation quickly and effectively.
Some patients may need:
- short courses during flare-ups,
- repeated courses,
- long-term low-dose treatment,
- inhaled steroid therapy,
- antifungal treatment,
- or biologic medicines to reduce the need for oral steroids.
For many patients, steroids are not optional or casual medicines. They may be essential treatments used to control serious inflammation and protect lung function.
Are steroids only meant for short-term use?
Patients sometimes hear that prednisolone was “only designed for short-term use”. This is understandable, because modern medical practice tries to avoid long-term steroid treatment where possible.
Long-term oral corticosteroids can cause significant side effects, including:
- adrenal suppression,
- diabetes or worsening blood sugar control,
- osteoporosis and fracture risk,
- increased infection risk,
- cataracts or glaucoma,
- muscle weakness,
- skin thinning and bruising,
- weight gain,
- sleep disturbance,
- and mood or mental health effects.
For this reason, doctors usually aim to use steroids at the lowest effective dose for the shortest safe time.
However, it is also important not to oversimplify this message. Some people with ABPA, severe asthma or other inflammatory lung conditions do need longer-term steroid treatment because the disease itself can be dangerous if not controlled.
In some patients, the risk of uncontrolled lung inflammation may outweigh the risks of steroid treatment, at least for a period of time.
Modern care increasingly tries to reduce steroid exposure by using other approaches where appropriate, such as:
- antifungal treatment,
- biologic medicines for severe asthma or ABPA-type inflammation,
- careful monitoring of lung function and blood tests,
- gradual steroid tapering,
- bone protection where needed,
- diabetes monitoring,
- and regular review of whether the steroid dose can be reduced.
The key message is not that patients have done anything wrong by needing steroids. The key message is that long-term steroid treatment deserves careful monitoring, honest discussion and regular review.
Patient reassurance: If you have needed prednisolone for ABPA or severe asthma, this does not mean you have failed or made a poor choice. It usually means your medical team has been trying to control a potentially serious inflammatory condition. The aim is to balance benefit and risk as safely as possible.
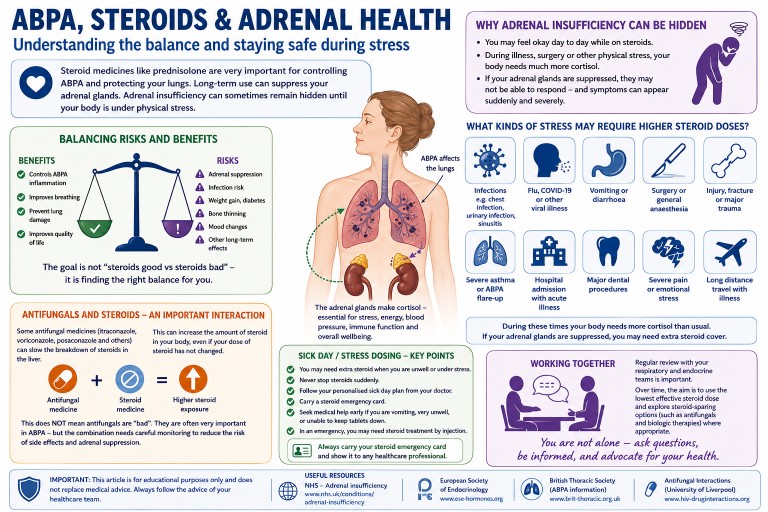
Balancing risks and benefits
One of the hardest parts of long-term steroid treatment is that two important things can be true at the same time:
- steroids can cause serious side effects,
- and steroids can also prevent serious lung damage and dangerous flare-ups.
Patients sometimes feel guilty, frustrated or frightened when they hear about the risks of prednisolone. Others may feel judged for “still being on steroids”.
However, many people with ABPA or severe asthma did not choose steroids lightly. Steroids are often prescribed because uncontrolled inflammation itself can damage the lungs, worsen bronchiectasis, increase hospital admissions and significantly reduce quality of life.
Modern respiratory care increasingly tries to reduce steroid exposure where possible using:
- antifungal therapy,
- biologic medicines,
- careful monitoring,
- gradual tapering plans,
- and better recognition of steroid side effects.
But for some patients, steroids may still remain an important part of treatment, even if the goal is eventually to reduce the dose.
The most helpful approach is usually not “steroids are good” or “steroids are bad”, but rather:
- What dose is truly needed?
- Can the dose be safely reduced?
- Are side effects being monitored properly?
- Are there alternative treatments available?
- And is the patient being listened to when symptoms change?
This balanced approach is increasingly recognised as one of the most important parts of caring for people with severe asthma and aspergillosis.
How steroids affect the body’s natural hormone system
Steroid medicines act in ways that are similar to natural cortisol.
When the body senses steroid medication in the bloodstream, it may reduce its own ACTH production. Over time, this can mean:
- ACTH falls,
- the adrenal glands become less active,
- and natural cortisol production decreases.
Doctors sometimes describe this as the adrenal glands “going to sleep”.
This is called:
- adrenal suppression,
- steroid-induced adrenal insufficiency,
- or hypothalamic-pituitary-adrenal axis suppression.
What is adrenal suppression?
Adrenal suppression means the body may not produce enough cortisol when it is needed.
This can become especially important during:
- infection,
- surgery,
- injury,
- severe stress,
- or rapid steroid reduction.
Some patients develop symptoms gradually. Others notice problems when trying to reduce steroid doses.
Because cortisol is part of the body’s stress response, people with adrenal insufficiency may need specific medical advice about what to do during illness, vomiting, surgery or severe infection.
Why symptoms can be difficult to recognise
Symptoms of adrenal suppression can overlap with many other conditions common in people with aspergillosis, ABPA or severe asthma.
Possible symptoms include:
- profound tiredness,
- weakness,
- dizziness,
- sweating,
- shakiness,
- nausea,
- muscle aches,
- low mood,
- brain fog,
- reduced exercise tolerance,
- poor recovery after illness,
- or feeling suddenly much worse after reducing steroids.
These symptoms may also occur with:
- an ABPA flare,
- asthma worsening,
- lung infection,
- chronic illness,
- poor sleep,
- anxiety,
- or steroid withdrawal.
This overlap is one reason why patients can feel frustrated or uncertain. Symptoms are real, even when the cause is difficult to pin down.
Why blood tests can become confusing
Many patients expect blood tests to give clear answers, but cortisol and ACTH results are often complicated.
Several things can affect results:
- time of day,
- recent steroid use,
- the type of steroid used,
- inhaled steroid dose,
- recent dose reductions,
- illness or stress,
- laboratory methods,
- and antifungal medicines.
Typical patterns
In classic steroid-induced adrenal suppression:
- cortisol is low,
- and ACTH is low or “inappropriately normal”.
This happens because steroid medication suppresses ACTH production.
However, real-life cases are not always straightforward. Some patients may have recently reduced steroids, missed doses, changed steroid type, used high-dose inhaled steroids, or taken antifungal medicines that alter steroid metabolism.
In some situations, endocrinologists may need repeated testing or dynamic tests such as a Synacthen test to understand whether the adrenal glands can respond properly.
It is important that patients do not try to interpret cortisol or ACTH results in isolation. The result needs to be understood alongside symptoms, medication history, timing of the sample and the clinical situation.
The role of inhaled steroids
Many people assume inhaled steroids only affect the lungs.
Inhaled steroids usually have fewer whole-body effects than long-term oral steroids, but high doses can sometimes contribute to adrenal suppression, especially when combined with:
- long-term or repeated oral steroid courses,
- azole antifungal medicines,
- other medicines that affect steroid metabolism,
- or individual differences in how medicines are processed.
This does not mean inhaled steroids are unsafe or should be stopped suddenly. For many people with asthma or ABPA, inhaled steroids are an important part of keeping airway inflammation under control.
It does mean that total steroid exposure should be reviewed carefully, especially in patients with symptoms suggestive of adrenal suppression.
Antifungal medicines and steroid interactions
This is an especially important issue in aspergillosis.
Antifungal medicines such as:
- itraconazole,
- voriconazole,
- posaconazole,
- and isavuconazole
can interact with other medicines, including corticosteroids.
Some azole antifungals slow the breakdown of steroids in the liver. This can increase the body’s exposure to steroid medication, meaning that even doses which initially appear moderate may sometimes behave more like higher doses inside the body.
This interaction may increase the risk of:
- adrenal suppression,
- Cushing-like side effects,
- weight gain,
- skin thinning,
- easy bruising,
- high blood sugar,
- muscle weakness,
- or hormonal imbalance.
The interaction can be particularly important in patients taking:
- oral prednisolone or methylprednisolone,
- high-dose inhaled steroids,
- multiple steroid preparations together,
- or repeated steroid courses over time.
Some patients tolerate steroid treatment reasonably well for long periods before antifungal medicines are added. Endocrine problems may then become more noticeable later, especially during:
- infection,
- surgery,
- vomiting or diarrhoea,
- major physical stress,
- rapid steroid reduction,
- or severe asthma or ABPA flare-ups.
This can feel as though adrenal insufficiency has appeared “suddenly” or “out of nowhere”, when in reality the adrenal glands may have been partially suppressed for some time.
Why adrenal insufficiency may only become obvious during illness or stress
Some patients with steroid-related adrenal suppression cope reasonably well during normal day-to-day life, especially while still taking regular steroids. However, the problem may become much more noticeable when the body faces significant physical stress.
Under normal circumstances, the body rapidly increases cortisol production during severe illness or injury. If the adrenal glands cannot respond properly, symptoms may suddenly become much more severe.
Patients sometimes describe:
- “crashing” during an infection,
- extreme exhaustion,
- severe weakness,
- dizziness or collapse,
- poor recovery after illness,
- or feeling suddenly unable to cope physically.
This does not mean every severe illness in an ABPA patient is caused by adrenal insufficiency. Infections, inflammation and lung disease themselves are often the major problem. However, adrenal suppression can sometimes contribute to deterioration and may only reveal itself during periods of stress or acute illness.
This is one reason why some patients are given “sick day rules”, emergency steroid cards or advice about temporary steroid dose increases during illness.
Importantly, this does not mean antifungal medicines are “bad” or should be avoided. In many patients, antifungal treatment significantly improves ABPA control and may eventually help reduce steroid exposure overall. The important message is that these combinations require awareness, monitoring and careful medical supervision.
Patients should never stop antifungal or steroid medicines suddenly without medical advice.
Steroid withdrawal versus adrenal insufficiency
Steroid withdrawal and adrenal insufficiency can feel very similar.
Steroid withdrawal
When steroid doses are reduced, the body may take time to adjust. Patients can temporarily feel unwell even if the adrenal glands are slowly recovering.
Adrenal insufficiency
Adrenal insufficiency means the body cannot produce enough cortisol to meet its needs.
Symptoms may overlap considerably. Recovery can sometimes take weeks or months, and in some patients longer.
For many patients, one of the hardest parts is that they may “look well” externally while feeling exhausted internally.
It is important that symptoms are not dismissed simply because they are difficult to measure.
What kinds of stress may require higher steroid doses?
Patients who have adrenal insufficiency or significant adrenal suppression may sometimes be advised to temporarily increase steroid doses during periods of physical stress. This is often called following “sick day rules”.
The body normally produces extra cortisol during stress, illness or injury. If the adrenal glands cannot respond properly, extra steroid medication may sometimes be needed to prevent serious illness.
Examples of situations that may place significant stress on the body include:
- high fever or significant infection,
- chest infection or pneumonia,
- vomiting or diarrhoea,
- COVID-19 or influenza,
- major dental treatment or surgery,
- fractures or significant injury,
- general anaesthetic procedures,
- severe asthma attacks or ABPA flare-ups,
- hospital admission with acute illness,
- or severe physical exhaustion associated with illness.
The exact advice varies between patients depending on:
- whether adrenal insufficiency has been formally diagnosed,
- the steroid dose currently being taken,
- how suppressed the adrenal glands are thought to be,
- other medical conditions,
- and guidance from endocrine or respiratory specialists.
Some patients are provided with:
- specific “sick day rules”,
- an emergency steroid card,
- medical alert jewellery,
- or emergency hydrocortisone injection kits.
Patients should only adjust steroid doses according to the advice provided by their medical team. If severe vomiting, collapse, confusion, inability to keep medication down or major deterioration occurs, urgent medical advice is needed.
When should patients seek urgent medical advice?
Patients should seek urgent medical help if they experience:
- collapse,
- fainting,
- severe vomiting,
- inability to keep steroid medication down,
- severe dehydration,
- confusion,
- severe weakness,
- very low blood pressure,
- or sudden major deterioration during illness.
These symptoms can occasionally indicate adrenal crisis, which is a medical emergency.
Patients who have been told they are at risk of adrenal insufficiency should follow the emergency and “sick day” advice given by their endocrine or respiratory team.
Frequently asked questions
Does everyone taking steroids develop adrenal suppression?
No. Risk depends on factors such as dose, duration, repeated courses, inhaled steroid dose, other medicines and individual sensitivity.
Can adrenal function recover?
Yes. Many patients gradually recover adrenal function over time, although recovery speed varies.
Are inhaled steroids safer than tablets?
Inhaled steroids usually have fewer whole-body effects than long-term oral steroids, but high doses can still contribute to adrenal suppression in some patients, especially when combined with certain antifungal medicines.
Why do I feel worse when reducing steroids?
This can happen for several reasons. The underlying lung disease may flare, the body may be adjusting to lower steroid levels, or cortisol production may not yet have recovered.
Does needing long-term prednisolone mean something has gone wrong?
Not necessarily. Long-term prednisolone is usually avoided where possible because of side effects, but some patients need it to control serious inflammation. The aim is regular review, careful monitoring and dose reduction when it is safe.
Should I stop steroids because of this risk?
No patient should stop prescribed steroids suddenly unless specifically advised by their medical team. Sudden withdrawal can be dangerous, especially if the body’s own cortisol production is suppressed.
Final thoughts
Adrenal suppression and steroid-related hormone problems are recognised complications of corticosteroid treatment.
For patients with aspergillosis, ABPA and severe asthma, the situation can become especially complex because:
- steroid treatment may be medically necessary,
- symptoms overlap with many other conditions,
- antifungal medicines may interact with steroids,
- inhaled steroids may add to total steroid exposure,
- and blood tests are not always straightforward.
Patients sometimes feel frustrated because their symptoms are difficult to explain or measure clearly. However, these experiences are recognised by clinicians and researchers, and steroid-related adrenal problems are increasingly acknowledged as important and sometimes under-recognised.
The goal is not to create fear of steroids. The goal is to use them carefully, monitor them properly, reduce them when possible, and support patients through the difficult process of balancing disease control with treatment side effects.
Suggested internal links
- ABPA treatment overview
- Steroid side effects
- Antifungal drug interactions
- Fatigue and aspergillosis
- Severe asthma and biologics
- Living with long-term aspergillosis
- Mental wellbeing and chronic illness
- Aspergillosis.org Knowledge Hub
References and further reading
When was this article last reviewed?
Last reviewed: May 2026
Author and review information
Prepared for patient education and support purposes.
This article is intended for general educational use and should not replace personalised medical advice from a healthcare professional.

Latest News posts
News archive