Steroids
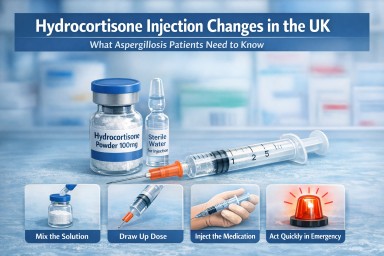
Hydrocortisone Injection Changes in the UK: What It Means for Aspergillosis Patients
Last reviewed: March 2026…




🌿 Your Immune System, Biologics, and Steroids: What’s Suppressed — and What Stays Strong
A clear, reassuring guide for…


Last reviewed: March 2026…
A clear, reassuring guide for…