Conditions


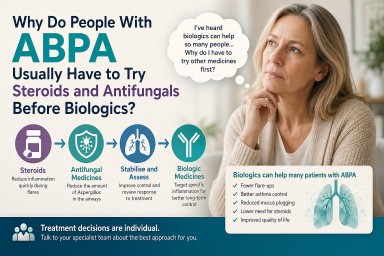
Why Do People With ABPA Usually Have to Try Steroids and Antifungals Before Biologics?
Last reviewed: June 2026…

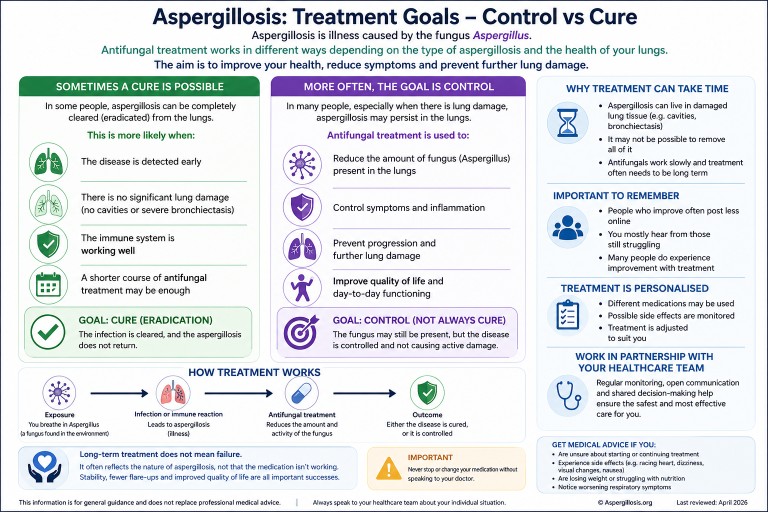
Can Aspergillosis Be Cured? Understanding Treatment, Control, and Long-Term Therapy
Last reviewed: April 2026…
Last reviewed: June 2026…
Last reviewed: April 2026…