Conditions
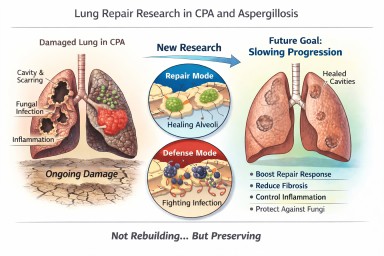
Looking further into the future - could we control lung damage, preserve healthy lung tissue better?
Can Lungs Repair Themselves?…
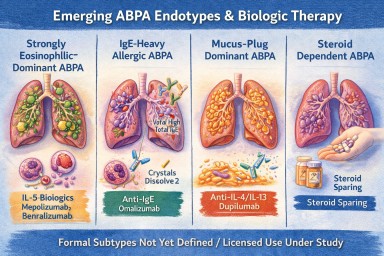
Invitation: Patient & Carer Discussion on Living with ABPA. New type of treatment.
🕙 10:00am, Thursday 12th Get…

Can blood tests help predict if chronic pulmonary aspergillosis will come back?
This study from the National…