Browse information
Latest Articles
Support
For Professionals
Search
Blood Tests
Home
Diagnostics
Archive by Category "Blood Tests"
Blood Tests
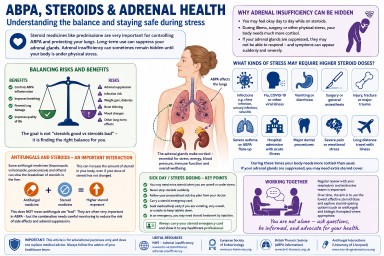
Understanding Steroids, Cortisol, ACTH and Adrenal Suppression in Aspergillosis
by GAtherton
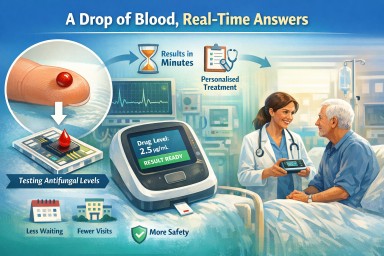
A Drop of Blood, Real-Time Answers
Last reviewed: 20 March……
by GAtherton
Can blood tests help predict if chronic pulmonary aspergillosis will come back?
This study from the National…
by GAtherton
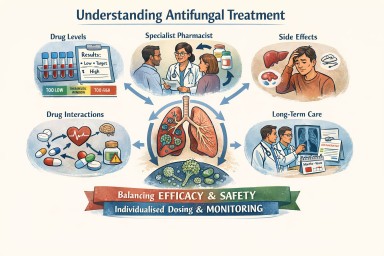
Antifungal Medicines: Dosing, Monitoring, and the Role of Specialist Care
A detailed reference for…
by GAtherton