Understanding how they work, when they’re helpful, and when extra care is needed
Biologic medicines (such as omalizumab, mepolizumab, benralizumab, dupilumab and newer options like tezepelumab) are increasingly used to treat Allergic Bronchopulmonary Aspergillosis (ABPA) and severe asthma. They can be life-changing for some people.
However, their place in Chronic Pulmonary Aspergillosis (CPA) — especially in people who have both ABPA and CPA together — is more complicated and needs careful specialist supervision.
This article explains what we know so far.
🌟 1. ABPA and CPA are different conditions — but some people have both
-
ABPA is mainly an allergic reaction to Aspergillus in the airways.
-
CPA is a chronic fungal infection that causes cavities, scarring, and long-term lung damage.
-
Some people start with ABPA and later develop CPA, or the two conditions overlap.
-
The 2024 international ABPA guidelines now recognise this overlap as real and important.
Because biologics target allergy pathways rather than fungal infection, treatment decisions must look at both sides of the disease.
🌿 2. Biologics in ABPA: the evidence is strong and growing
Biologics can help patients with ABPA or severe asthma by:
-
reducing steroid use
-
improving breathing
-
decreasing mucus plugging
-
lowering flare-ups
-
improving quality of life
Biologics most commonly used in ABPA include:
| Biologic | Target | Notes |
|---|---|---|
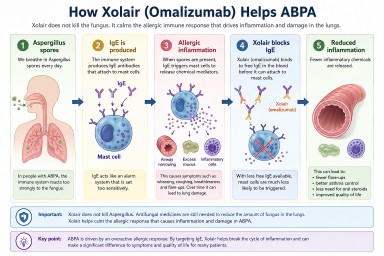
| Omalizumab | IgE | Well established, helps many ABPA patients |
| Mepolizumab | IL-5 | Helps eosinophilic inflammation |
| Benralizumab | IL-5Rα | Similar to mepolizumab; long-acting |
| Dupilumab | IL-4Rα | Very promising for allergic disease; growing evidence for ABPA |
| Tezepelumab | TSLP | Very new; limited ABPA data so far |
For many people with ABPA, biologics are safe and effective when monitored.
⚠️ 3. Biologics and CPA: much less evidence
-
CPA is caused by persistent fungal infection and structural lung damage.
-
Biologics do not treat fungal infection, and they do not prevent cavities.
-
In CPA, the mainstay of treatment is still:
-
antifungal medication (usually itraconazole, voriconazole or posaconazole)
-
careful imaging (CT scans)
-
airway clearance
-
sometimes surgery or bronchoscopy
-
There is no strong evidence that biologics help CPA itself.
🔄 4. What about patients who have both ABPA and CPA?
This is where things become more complex.
Biologics may help the allergic part (ABPA), but:
-
they do not treat fungal infection
-
they do not stop fungal cavities from progressing
-
they may reduce inflammation that normally helps the body contain infection
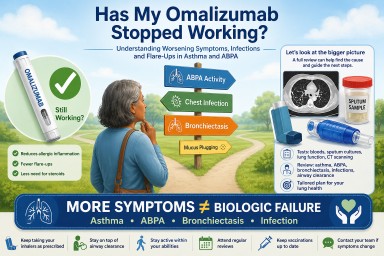
If antifungal treatment is interrupted or not strong enough, fungal activity may increase while the allergic symptoms improve — so regular monitoring is essential.
Specialist centres (like the NAC) now emphasise:
✔️ Continue antifungals if CPA is active
✔️ Watch cavities with regular CT scans
✔️ Monitor Aspergillus IgG/IgE and fungal cultures
✔️ Check whether symptoms are from allergy, infection, or both
✔️ Make joint plans between asthma/airway doctors and mycology specialists
❓ 5. Are some biologics better than others for ABPA/CPA overlap?
There is no official guidance yet, but early observations suggest:
⭐ Most promising for ABPA:
-
Dupilumab seems particularly effective for allergic disease (IgE, mucus, airflow), though still off-label for ABPA.
⭐ Increasing interest:
-
Tezepelumab works outside the eosinophil pathway and may be useful in some asthma types, but research in ABPA is only just starting.
⭐ Useful in selected cases:
-
Anti-IL-5 biologics (mepolizumab, benralizumab) help airway eosinophils but may not help every ABPA patient.
⚠️ Uncertain in CPA:
-
None of the biologics treat fungal infection or cavities directly.
-
Their role in active CPA remains unclear and requires careful oversight.
🧭 6. What this means for patients
If you have ABPA only, biologics may be an excellent option — especially if:
-
steroids cause side-effects
-
your asthma is uncontrolled
-
you have frequent flare-ups
-
your IgE levels are very high
-
mucus plugging or wheezing continues despite treatment
If you have CPA or cavities, treatment needs to be more cautious:
-
antifungal medication usually needs to continue
-
biologics may still help if the allergic component is significant
-
CT scans must be repeated to make sure cavities are not progressing
-
specialists must weigh benefits vs. risk for each patient individually
💬 7. Summary
-
Biologics can be extremely helpful for ABPA.
-
They do not treat CPA, and cannot replace antifungal medicines.
-
In patients with both ABPA and CPA, the approach must be personalised.
-
Dupilumab and (possibly) tezepelumab are emerging biologics with promise, but evidence is still developing.
-
Decisions should always be made with a specialist centre such as the National Aspergillosis Centre (NAC).