Many people with severe asthma or Allergic Bronchopulmonary Aspergillosis (ABPA) now have access to biologic medicines — treatments that block very specific signals in the immune system. For some, the results can feel miraculous. For others, the effect may fade or never fully take hold. But the exciting news is that science is building a toolkit of biologics that can be matched more closely to each person.
✨ Why biologics sometimes stop working
-
Biologics like tezepelumab (which blocks TSLP) can give dramatic improvements, but in some people the benefit doesn’t last.
-
That may be because the immune system “switches pathways” — other signals (like IL-5 or IL-13) start to dominate.
-
It doesn’t mean treatment is over — it means we need to try a different tool in the kit.
🧰 The current toolkit
Each biologic blocks a different “messenger” (called cytokines) in the immune system:
-
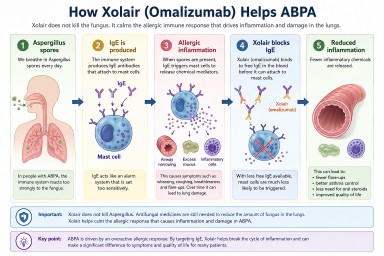
IgE blocker (omalizumab): helps in allergy-driven asthma/ABPA.
-
IL-5 / IL-5R blockers (mepolizumab, benralizumab, reslizumab, and soon depemokimab): reduce eosinophils (a type of white blood cell) that cause inflammation.
-
IL-4 / IL-13 blocker (dupilumab): controls type-2 inflammation, also helpful in eczema and nasal polyps.
-
TSLP blocker (tezepelumab): targets an “alarmin” high up in the pathway, useful across many asthma types.
-
IL-33 blockers (in development): another upstream “alarmin” that could help in the future.
🚀 What’s new and coming soon
-
Depemokimab: a long-acting IL-5 treatment, given only twice a year.
-
Inhaled anti-TSLP: same target as tezepelumab, but in inhaler form.
-
IL-33 blockers: still experimental, but promising because IL-33 is involved in fungal allergy and ABPA.
💡 What this means for ABPA
-
ABPA involves allergy (IgE), eosinophils (IL-5), and other signals like IL-33.
-
That’s why some patients respond to omalizumab, others to mepolizumab/benralizumab, others to dupilumab, and some to tezepelumab.
-
In the future, doctors may be able to choose the exact biologic (or even combination) that best matches your immune profile — just like targeted cancer treatments today.
🧩 The Biologic Toolkit (summary table)
| Target Signal | Biologics | How it Helps | Relevance to ABPA |
|---|---|---|---|
| IgE (allergy antibody) | Omalizumab | Calms allergic reactions | Useful when IgE is high and fungus/allergy is a trigger |
| IL-5 / IL-5R (eosinophils) | Mepolizumab, Benralizumab, Reslizumab, Depemokimab (6-monthly) | Reduces eosinophils that damage lungs | Helpful in many ABPA patients with high eosinophils |
| IL-4 / IL-13 (type-2 inflammation) | Dupilumab | Reduces mucus, inflammation, and steroid need | Good in patients with eczema or nasal polyps alongside ABPA |
| TSLP (alarmin, upstream trigger) | Tezepelumab, Inhaled anti-TSLP (in trials) | Blocks an “early alarm” that activates many asthma pathways | Early evidence: big improvements in some ABPA patients |
| IL-33 / ST2 (alarmin) | Itepekimab, Astegolimab (in development) | Switches off another early “danger signal” | IL-33 is strongly linked to fungal allergy → promising for ABPA |
🫁 COPD, Bronchiectasis & Mucus Plugging
-
COPD: Some biologics (like anti-IL-5) show benefit in patients with high eosinophils, and IL-33 blockers are being tested. Not yet routine NHS use.
-
Bronchiectasis: Biologics mainly help when asthma/ABPA overlap is present. Airway infections remain the bigger challenge.
-
Mucus plugging: Dupilumab can reduce mucus production. Other biologics may help indirectly, but airway clearance techniques remain essential.
💷 Why new medicines are expensive
-
Developing a new drug takes 10–15 years and can cost over £1 billion.
-
Most drugs fail — profits from a few successes must cover all the failures.
-
Patents give companies a period of exclusivity to recover costs, after which cheaper copies (generics or biosimilars) appear.
📊 Open market vs NHS
-
In the US (open market), companies set prices, and insurers or patients decide if they can pay → faster access, but very high costs and inequality.
-
In the UK (NHS), the system is funded by taxpayers. NICE weighs up cost vs benefit before approving drugs → slower access sometimes, but once approved, everyone gets it fairly.
🧬 Rare diseases and fungal infections
-
For rare diseases like ABPA and CPA, the market is too small to attract big pharma on profit alone.
-
Organisations like GAFFI (Global Action for Fungal Infections) and DNDi (Drugs for Neglected Diseases initiative) work with universities, charities, and governments to develop antifungals.
-
Examples:
-
Olorofim (F2G, UK biotech): a brand-new antifungal class, developed with public and charity support.
-
Rezafungin: a long-acting antifungal supported by government and public funding.
-
-
Without these partnership models, fungal drugs for ABPA/CPA would likely not exist.
🌈 The takeaway
-
Biologics are transforming treatment for asthma and ABPA — and new ones are coming.
-
If one biologic doesn’t work, others may.
-
COPD, bronchiectasis, and mucus plugging may also benefit in future.
-
New drugs are costly to develop, but the NHS negotiates to keep access fair.
-
For rare diseases like ABPA/CPA, partnerships and advocacy are crucial to get new drugs developed at all.
📖 Glossary of Acronyms
ABPA – Allergic Bronchopulmonary Aspergillosis
A lung condition caused by allergy to Aspergillus fungus, leading to inflammation, mucus plugging, and lung damage.
CPA – Chronic Pulmonary Aspergillosis
A long-term lung infection with Aspergillus fungus, usually in people with existing lung disease.
COPD – Chronic Obstructive Pulmonary Disease
A group of lung conditions (like chronic bronchitis and emphysema) that cause breathing difficulties.
NHS – National Health Service
The publicly funded healthcare system in the UK.
NICE – National Institute for Health and Care Excellence
The body that decides which treatments the NHS should fund, based on cost and benefit.
QALY – Quality-Adjusted Life Year
A way of measuring the benefit of a treatment: how much it improves both the length and quality of life.
IL – Interleukin
A type of messenger protein (cytokine) used by the immune system to trigger inflammation. Different ILs have numbers (IL-4, IL-5, IL-13, IL-33).
IgE – Immunoglobulin E
An antibody linked to allergies. Very high IgE levels are common in asthma and ABPA.
TSLP – Thymic Stromal Lymphopoietin
An “alarmin” (early danger signal) that tells the immune system to start reacting. Blocked by tezepelumab.
ST2 – Suppression of Tumorigenicity 2
The receptor for IL-33. Drugs like astegolimab block this pathway.
GAFFI – Global Action For Fungal Infections
A non-profit organisation pushing for better care, awareness, and research into fungal disease.
DNDi – Drugs for Neglected Diseases initiative
An international group that develops treatments for rare or overlooked diseases (including fungal infections).
EAMS – Early Access to Medicines Scheme
A UK programme that allows patients to use promising medicines before full approval.
FDA / EMA / MHRA – Food and Drug Administration (US) / European Medicines Agency (EU) / Medicines and Healthcare products Regulatory Agency (UK)
The agencies that approve and regulate medicines.