Browse information
Latest Articles
Support
For Professionals
Search
Research
Home
Archive by Category "Research"
Research
Carriers of cystic fibrosis may be at greater risk for allergic bronchopulmonary aspergillosis
by GAtherton
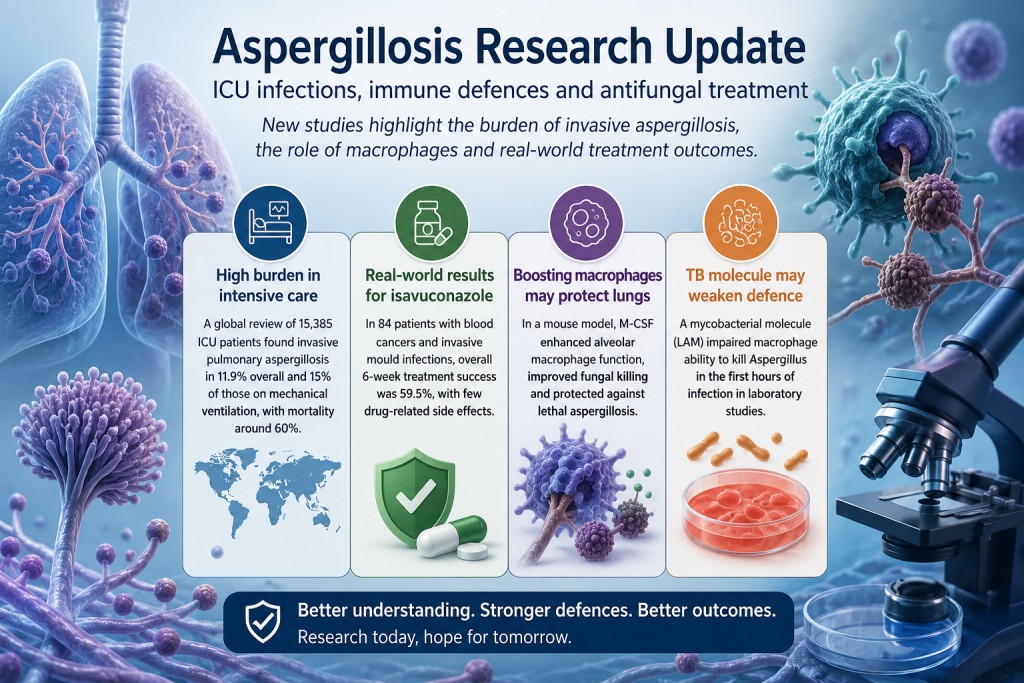
Aspergillosis Research Update: ICU Infections, Immune Defences and Antifungal Treatment
by GAtherton
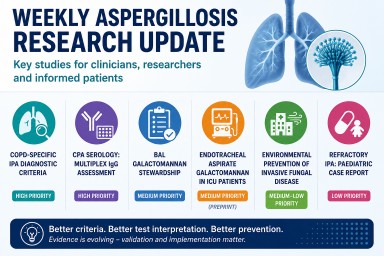
Weekly Aspergillosis Research Update: COPD IPA Criteria, CPA Serology, ICU Galactomannan and Environmental Prevention
by GAtherton
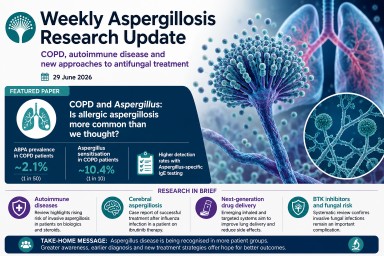
Weekly Aspergillosis Research Update: June 29
by GAtherton
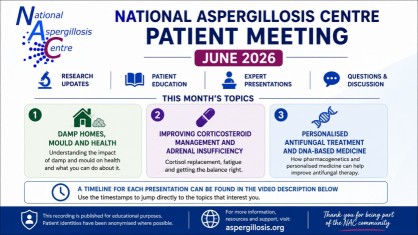
Catch Up on the Latest National Aspergillosis Centre Monthly Update
DNA Diagnostics, Adrenal…
by GAtherton
Weekly Aspergillosis Research Update: New Diagnostics, CAPA Evidence, and Why Azole Tolerance Matters
by GAtherton
Weekly Aspergillosis Research Update – 15 June 2026
by GAtherton
Professional Aspergillosis Update: May 2026
Audience: respiratory…
by GAtherton
Clinical Trials Update: Progress in ABPA and Invasive Aspergillosis Research
by GAtherton
Aspergillosis Research Update: Week Ending 8 June 2026
Key Points This was a…
by GAtherton
1
2
3
…
14