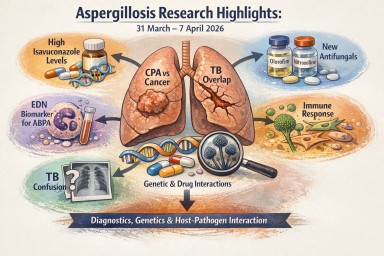
This week’s papers point in…
by GAtherton
Last reviewed: April 2026…
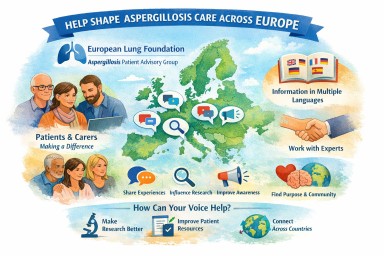
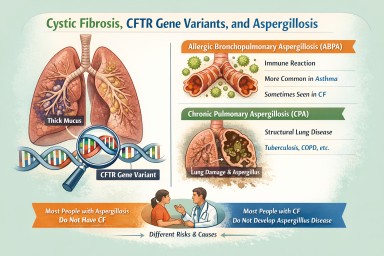
Many people living with…
Last reviewed: 8 April 2026…
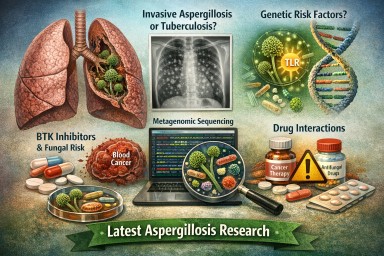
This week’s research…
Contents Key highlights 1.…
Last reviewed: 24 March 2026…
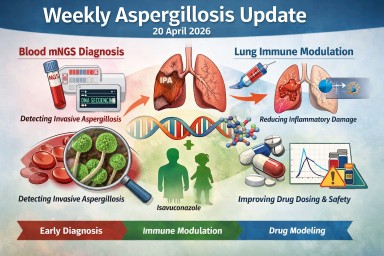
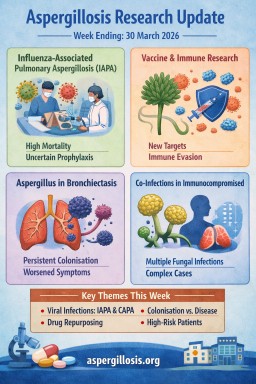
This week’s aspergillosis…
Last reviewed: 20 March……