Research

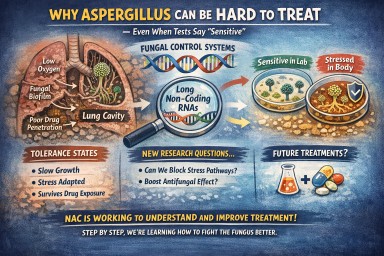
Why Can Aspergillus Infection Be Hard to Clear — Even When Tests Say It’s “Sensitive”?
Many patients ask: “If my…
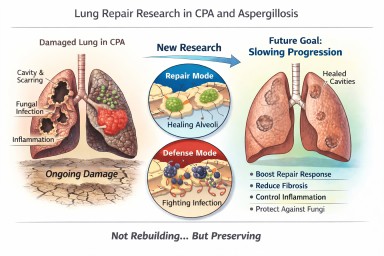
Looking further into the future - could we control lung damage, preserve healthy lung tissue better?
Can Lungs Repair Themselves?…
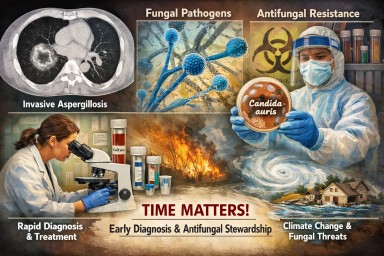
Systemic fungal infections: why speed, diagnosis and stewardship matter
Systemic fungal infections —…