Allergic Bronchopulmonary Aspergillosis (ABPA) can be confusing. It is often described as an allergic condition, yet patients may also be told there is “fungus in the lungs”.
In reality, both can be true at the same time.
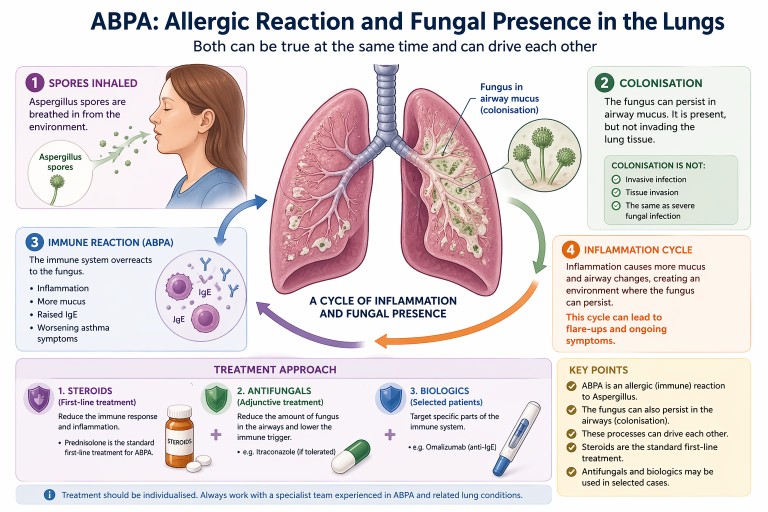
Key points
- ABPA is primarily an allergic (immune) reaction to Aspergillus
- The fungus can also persist in the airways (colonisation)
- Colonisation is not the same as invasive infection
- Steroids are the standard first-line treatment
- Antifungals and biologics may be used in selected cases
What is ABPA?
ABPA is a condition where the immune system overreacts to a common environmental fungus, most often Aspergillus fumigatus.
For a full introduction, see our guide to
what is ABPA.
This leads to:
- airway inflammation
- increased mucus production
- worsening asthma symptoms
- raised Immunoglobulin E (IgE) levels
If you are unfamiliar with IgE, see
our explanation of IgE.
Importantly, ABPA is not an invasive fungal infection. The lungs are reacting to fungal material rather than being invaded by it.
Can the fungus live in the lungs?
Yes—this is an important nuance.
In people with conditions such as:
- asthma
- bronchiectasis
the structure of the airways can allow Aspergillus to persist in mucus within the airways. This is known as colonisation.
Colonisation means:
- the fungus is present in airway mucus
- it may grow at low levels locally
- it does not invade lung tissue
This is very different from serious invasive fungal infections seen in severely immunocompromised patients.
How ABPA and colonisation interact
ABPA and colonisation are best understood as part of a spectrum of Aspergillus-related lung disease.
They can interact in a cycle:
- Aspergillus spores are inhaled
- The fungus persists in airway mucus
- The immune system reacts strongly (ABPA)
- Inflammation leads to more mucus production
- This creates an environment where the fungus can persist
This cycle can contribute to:
- recurrent flare-ups
- ongoing inflammation
- persistently raised IgE levels
Standard treatment: steroids
Oral corticosteroids are the traditional first-line treatment for ABPA.
Steroids such as prednisolone are used because they:
- reduce airway inflammation
- suppress the allergic immune response
- improve symptoms such as breathlessness and cough
- help control flare-ups
Learn more in our guide to
steroids and aspergillosis.
Where do antifungals fit in?
Antifungal medications such as itraconazole are often used as an additional (adjunctive) treatment rather than the primary therapy.
The aim is to:
- reduce the amount of fungus present in the airways
- lower the trigger for the immune response
- sometimes allow a reduction in steroid dose
For more detail, see our
antifungal treatments guide.
Biologic treatments
Biologic therapies such as omalizumab (anti-IgE) are increasingly used in some patients, particularly when:
- symptoms are difficult to control
- steroid side effects are significant
- there is severe asthma alongside ABPA
Read more about
biologics in asthma and ABPA.
Why results and symptoms may not match
Some people with ABPA may feel relatively well but still have:
- raised IgE levels
- evidence of fungal presence in the airways
This is because blood tests reflect underlying immune activity, which does not always match how a person feels day to day.
Why treatment is individualised
Although steroids are the standard treatment, management is often tailored to the individual. This is because people may also have:
- asthma
- bronchiectasis
- difficulty tolerating antifungal medications
- side effects from long-term steroid use
Specialist teams balance these factors when planning treatment.
When to seek medical advice
People with ABPA should seek medical review if they experience:
- worsening breathlessness
- increased cough or sputum
- new or persistent chest symptoms
- possible medication side effects
Treatment decisions should always be made with a clinician experienced in managing Aspergillus-related lung disease.
Summary
- ABPA is primarily an allergic condition
- The fungus can also persist in the airways (colonisation)
- These processes can drive each other
- Steroids are the standard first-line treatment
- Antifungals and biologics may be used in selected cases
Last reviewed: April 2026
Prepared by: National Aspergillosis Centre (patient information resource)

Latest News posts
News archive