Article type: Clinical and expert-patient evidence updateIntended audience: Ear, nose and throat clinicians, infectious diseases specialists, medical mycologists, general practitioners, specialist nurses, expert patients and carers.Last reviewed: June 2026
Key points
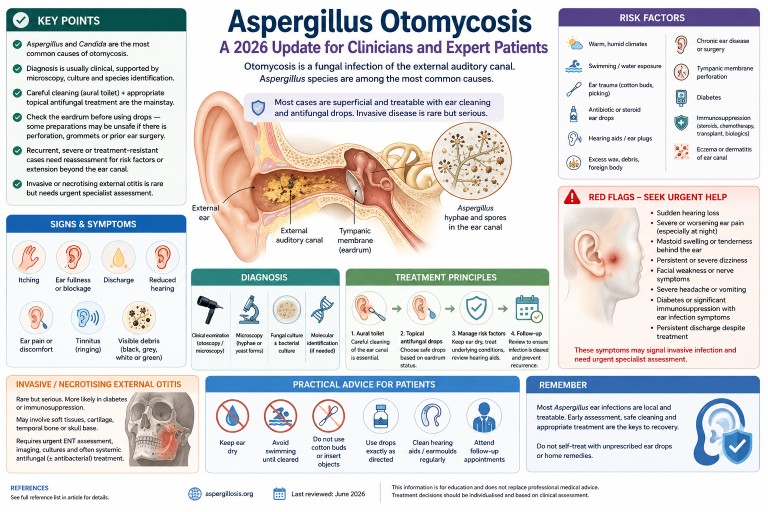
- Otomycosis is a fungal infection of the external auditory canal. It is often described as fungal otitis externa.
- Aspergillus species and Candida species are the most commonly reported causes.
- Older reports often describe Aspergillus niger as the main cause, but molecular methods show that related black Aspergillus species, including Aspergillus tubingensis, may previously have been misidentified as A. niger.
- Diagnosis is usually clinical, supported where possible by microscopy, fungal culture and species identification.
- Successful treatment usually requires careful cleaning of the ear canal as well as appropriate topical antifungal treatment.
- Before topical treatment is used, clinicians should assess whether the tympanic membrane is intact, because some preparations may be unsafe if there is perforation, grommets, a mastoid cavity or previous ear surgery.
- Most cases are superficial, but recurrent, severe or treatment-resistant disease should prompt reassessment for mixed bacterial infection, diabetes, immunosuppression, hearing aid moulds, foreign body, chronic ear disease or extension beyond the external canal.
- Invasive or necrotising external otitis is rare but serious and requires urgent specialist assessment.
- Sudden hearing loss, facial weakness, severe persistent pain, mastoid swelling or tenderness, neurological symptoms, or infection in a person with diabetes or significant immunosuppression should be treated as red flags.
Contents
- What is otomycosis?
- Aspergillus ear infection is different from lung aspergillosis
- Why Aspergillus matters
- Epidemiology and why cases may be missed
- Causative Aspergillus species
- Risk factors
- Symptoms and clinical features
- Diagnosis
- Differential diagnosis
- Treatment principles
- Recurrent or treatment-resistant otomycosis
- Invasive Aspergillus ear infection and necrotising external otitis
- Practical advice for patients
- Frequently asked questions
- When to seek urgent medical help
- Evidence gaps and uncertainty
- References
What is otomycosis?
Otomycosis is a fungal infection of the external auditory canal, the skin-lined passage leading from the outer ear to the eardrum. It is also called fungal otitis externa. The infection may be acute, subacute or chronic, and it can be mistaken for bacterial otitis externa, eczema, wax, chronic discharge or non-specific inflammation.
In most people, otomycosis is a superficial infection of the outer ear canal. It can be uncomfortable, persistent and prone to recurrence, but it is usually treatable when the ear is examined, cleaned and treated appropriately. Rarely, particularly in people with diabetes, immunosuppression, previous ear surgery or severe persistent symptoms, infection may spread beyond the ear canal and become invasive.
Plain-English summary: most Aspergillus ear infections affect the outer ear canal. They are usually not the same as invasive aspergillosis in the lungs or bloodstream, but they can still need specialist ear care to clear the infection safely.
Aspergillus ear infection is different from lung aspergillosis
Many people searching online for Aspergillus find information about chronic pulmonary aspergillosis, allergic bronchopulmonary aspergillosis or invasive aspergillosis. These are different conditions.
Aspergillus otomycosis usually affects the external ear canal only. It is usually a local fungal infection rather than a whole-body infection. It does not usually mean that a person has invasive aspergillosis, chronic pulmonary aspergillosis or allergic bronchopulmonary aspergillosis.
However, people with existing lung disease, diabetes, immune suppression or complex medical histories should still tell their clinician about these conditions, because they may affect assessment and treatment decisions.
Why Aspergillus matters
Aspergillus is a common environmental mould. Its spores are present in air, dust, soil, compost, decaying vegetation and indoor environments. In the ear canal, fungal growth is favoured when local conditions change. Moisture, trauma to the skin, loss of normal wax protection, altered acidity, previous antibiotic or steroid drops, retained debris and obstruction from hearing aid moulds or ear plugs can all make fungal overgrowth more likely.
In otomycosis, Aspergillus species are among the most frequently reported fungi. They are particularly important because their appearance in the ear can be striking, with black, grey, greenish, yellow-white or fluffy debris. However, appearance alone is not enough for precise species identification.
Epidemiology and why cases may be missed
Reported prevalence varies considerably between studies and geographical regions. Otomycosis is more common in some warm, humid or dusty environments, but it is reported worldwide, including in the United Kingdom. In UK practice, it may be considered particularly in chronic, recurrent or treatment-resistant otitis externa.
Cases may be missed because symptoms overlap with bacterial otitis externa and inflammatory ear conditions. A patient may be treated repeatedly with antibacterial or steroid-containing ear drops before fungal infection is considered. In some cases, antibacterial treatment may suppress bacteria while allowing fungi to overgrow.
A 2025 systematic review highlighted increasing use of molecular methods for species identification, although many published studies still rely primarily on microscopy and culture.
Causative Aspergillus species
Older articles often refer to Aspergillus niger as the dominant Aspergillus species in otomycosis. This remains a useful clinical shorthand, but it is no longer the whole story. Modern molecular identification has shown that black Aspergillus isolates are a complex group and may include species such as Aspergillus tubingensis and other members of the Aspergillus niger complex.
Reported Aspergillus species in otomycosis and fungal otitis externa include:
- Aspergillus niger complex, including related black Aspergillus species
- Aspergillus tubingensis
- Aspergillus flavus
- Aspergillus fumigatus
- Aspergillus terreus complex, reported occasionally in superficial infection series but apparently less common than the Aspergillus niger complex or Aspergillus flavus
Clinical relevance: species-level identification is not always needed for straightforward cases that respond to topical treatment. It becomes more important in recurrent, invasive, immunocompromised or treatment-resistant infection, or where systemic antifungal treatment is being considered.
Risk factors
Otomycosis usually develops when the normal protective environment of the ear canal is disrupted. Important risk factors include:
- warm, humid or dusty environments
- frequent swimming or repeated water exposure
- use of cotton buds, ear picking or other trauma to the ear canal
- previous or repeated antibacterial ear drops
- topical steroid use in the ear
- hearing aids, ear plugs or occlusive moulds
- excess wax, retained debris or foreign material
- chronic otitis externa or chronic otitis media
- previous ear surgery or mastoid cavity
- tympanic membrane perforation
- diabetes, especially if poorly controlled
- immunosuppression, including chemotherapy, transplant medicines, prolonged high-dose corticosteroids and some biological therapies
- skin conditions affecting the ear canal, such as eczema or seborrhoeic dermatitis
Plain-English summary: fungi grow more easily when the ear canal is damp, damaged, blocked, repeatedly treated with antibiotics, or when a person’s immune defences are reduced.
Symptoms and clinical features
Symptoms vary. Some patients have mild itching and fullness, while others have marked discomfort, discharge or hearing loss. Common symptoms include:
- itching in the ear
- ear fullness or blockage
- discharge from the ear
- reduced hearing, often due to debris blocking the canal
- ear discomfort or pain
- tinnitus or ringing in the ear
- scaling, inflammation or visible debris in the ear canal
Severe pain, persistent night pain, swelling around the ear, tenderness or swelling over the mastoid bone behind the ear, fever, persistent or severe dizziness, facial weakness, severe headache, cranial nerve symptoms or symptoms in a person with diabetes or immunosuppression should raise concern for more serious disease.
Sudden hearing loss should be treated as a medical emergency and assessed urgently, regardless of whether otomycosis is suspected.
Diagnosis
Clinical examination
Diagnosis is often suspected by otoscopic or microscopic examination of the ear canal. Typical findings may include fungal debris, spores, hyphae, wet or dry masses, inflammation, scaling, discharge and obstruction. Black, grey, white, yellow-green or fluffy material may be seen, but visual appearance does not reliably identify the species.
Assessment should include:
- extent of external canal inflammation
- presence of fungal debris or discharge
- degree of canal obstruction
- condition of the tympanic membrane
- evidence of perforation, grommets, mastoid cavity or prior surgery
- features suggesting bacterial co-infection
- signs of spread beyond the external canal
Microscopy and fungal culture
Microscopy can demonstrate fungal hyphae or yeast forms. Culture can identify whether Aspergillus, Candida or another fungus is present. Bacterial culture may also be useful if mixed infection is suspected.
Culture is especially helpful when disease is recurrent, severe, atypical, invasive, not responding to standard treatment, or occurring in a person with diabetes, immunosuppression or previous ear surgery.
Molecular identification
Molecular methods can identify Aspergillus species more accurately than morphology alone. This matters because older culture-based reports may have grouped several black Aspergillus species under Aspergillus niger. Molecular identification may also help in epidemiological studies and difficult clinical cases.
For routine mild otomycosis, molecular identification is not always necessary. For persistent, recurrent or invasive disease, species-level identification and antifungal susceptibility testing may help guide treatment.
Antifungal susceptibility testing
Antifungal susceptibility testing is not required for every simple case. It should be considered when there is treatment failure, recurrent disease, unusual species, invasive infection or planned systemic antifungal therapy. Susceptibility patterns may vary between Aspergillus species, although resistance testing is not routinely required for uncomplicated superficial disease.
When to consider imaging
Imaging is not needed for uncomplicated superficial otomycosis. It may be required if there is concern about necrotising external otitis, skull base osteomyelitis, mastoid involvement, middle ear extension, cranial nerve involvement or deep tissue spread. Imaging decisions should be made by ear, nose and throat, infectious diseases, radiology and microbiology or mycology specialists as appropriate.
Differential diagnosis
Conditions that can resemble Aspergillus otomycosis include:
- bacterial otitis externa
- chronic otitis externa
- eczema or dermatitis of the ear canal
- impacted wax
- foreign body
- chronic suppurative otitis media
- cholesteatoma
- otitis media with perforation
- necrotising external otitis
- malignancy of the external canal or temporal bone, rarely
Failure to respond to usual antibacterial treatment should prompt reconsideration of the diagnosis rather than repeated courses of the same treatment.
Treatment principles
Treatment depends on severity, tympanic membrane status, immune status, recurrence, species where known, and whether infection is limited to the outer ear canal. Local ear, nose and throat practice and local antimicrobial guidance should be followed.
1. Aural toilet and debridement
Careful cleaning of the ear canal is central to management. Fungal debris can block the canal, protect organisms from topical treatment and contribute to hearing loss. Aural toilet, often using microsuction or careful debridement, is usually best performed by a trained clinician using appropriate equipment, especially if the canal is swollen, painful, obstructed, or if the tympanic membrane cannot be seen.
Patients should not attempt deep cleaning with cotton buds, hair grips, ear candles or improvised tools. These can damage the ear canal, push debris deeper, worsen inflammation or perforate the eardrum.
Ear irrigation is not usually the preferred approach for suspected otomycosis, because retained moisture may encourage fungal growth and because irrigation may be unsafe if there is tympanic membrane perforation, grommets or previous ear surgery.
2. Topical antifungal treatment
Most uncomplicated otomycosis is treated with topical antifungal therapy after cleaning. Reported agents include clotrimazole, miconazole, nystatin, ciclopirox and other locally used preparations. Different countries and ear, nose and throat services use different formulations, and the evidence does not clearly establish one universally superior topical agent for all cases.
Choice of topical treatment should consider:
- likely organism: mould versus yeast
- whether the tympanic membrane is intact
- previous ear surgery, mastoid cavity or grommets
- local formulary and ear, nose and throat practice
- potential ototoxicity
- patient tolerance and adherence
- whether the canal needs repeat cleaning
3. Tympanic membrane safety
Assessment of the eardrum is important. Some topical agents, antiseptics, acidic preparations or combination drops may be unsafe if the tympanic membrane is perforated or if there are grommets, a mastoid cavity or previous ear surgery. If the eardrum cannot be visualised, treatment should be chosen cautiously and specialist ear, nose and throat advice may be needed.
Important safety point
Patients should not put unprescribed antifungal, antiseptic, acidic, oil-based or herbal preparations into the ear. This is especially important if there is discharge, severe pain, previous ear surgery, grommets, suspected perforated eardrum, sudden hearing loss, dizziness or facial weakness.
4. Mixed bacterial and fungal infection
Mixed infection can occur. If bacterial infection is suspected, bacterial culture and targeted antibacterial treatment may be needed. However, repeated broad-spectrum antibacterial drops without reassessment may encourage fungal overgrowth and delay recognition of otomycosis.
5. Hearing aids, earmoulds and ear plugs
Hearing aids, earmoulds and ear plugs can trap moisture and debris in the ear canal. They may also act as a continuing source of irritation or contamination if not cleaned properly. In recurrent otomycosis, hearing aids and moulds should be reviewed, cleaned according to manufacturer guidance and, where appropriate, assessed by audiology or ear, nose and throat services.
6. Diabetes and immune suppression
People with diabetes or significant immune suppression need particular care, because severe or invasive external ear infection is more likely in these groups. Optimising glycaemic control may help reduce the risk of severe or recurrent infection. Clinicians should consider whether persistent or severe otitis externa in a person with diabetes could represent necrotising external otitis.
7. Systemic antifungal treatment
Systemic antifungal treatment is not usually required for uncomplicated superficial otomycosis. It may be considered in selected situations, including:
- invasive or necrotising external otitis
- extension into the middle ear, mastoid, skull base or surrounding tissues
- severe infection in an immunocompromised patient
- persistent disease where topical therapy is not possible, unsafe or ineffective
- cases requiring multidisciplinary ear, nose and throat, infectious diseases and mycology input
Systemic antifungal choice should be guided by species identification, susceptibility testing, site and extent of infection, drug interactions, renal and liver function, and local specialist advice. Azole antifungals such as itraconazole, voriconazole, posaconazole and isavuconazole have important drug interactions and monitoring requirements.
Recurrent or treatment-resistant otomycosis
Recurrent otomycosis is common in some series. Recurrence does not always mean that the original treatment was wrong; it may reflect ongoing risk factors or incomplete clearance of debris.
When otomycosis recurs or fails to respond, clinicians should reassess:
- Was the ear canal adequately cleaned?
- Can the tympanic membrane be seen?
- Is there perforation, chronic otitis media or mastoid cavity disease?
- Is there a hearing aid mould, ear plug or foreign body contributing?
- Is the patient using cotton buds or self-cleaning the ear?
- Is there persistent water exposure?
- Is there eczema, dermatitis or another inflammatory ear condition?
- Is there mixed bacterial and fungal infection?
- Has microscopy or culture confirmed the organism?
- Is species-level identification or susceptibility testing needed?
- Is the patient diabetic or immunocompromised?
- Is there severe pain, mastoid tenderness or evidence of deeper spread?
Invasive Aspergillus ear infection and necrotising external otitis
Most Aspergillus otomycosis is superficial. However, fungal infection of the external ear can rarely become invasive, particularly in people with diabetes, immunosuppression, severe chronic ear disease or previous ear surgery.
Necrotising external otitis, historically called malignant external otitis, is a severe infection that may involve soft tissues, cartilage, temporal bone or skull base. It is most often bacterial, especially due to Pseudomonas aeruginosa, but fungal cases including Aspergillus and Candida are reported. Fungal necrotising external otitis can be difficult to diagnose and may require prolonged treatment.
Features that should raise concern include:
- severe, persistent or worsening ear pain, especially at night
- pain out of proportion to examination findings
- persistent discharge despite appropriate treatment
- granulation tissue in the ear canal
- facial weakness or other cranial nerve symptoms
- persistent, severe or worsening dizziness, particularly with severe pain, hearing loss or neurological symptoms
- severe headache or neurological symptoms
- swelling, redness or cellulitis around the ear
- tenderness, swelling or redness over the mastoid bone behind the ear
- diabetes, especially if poorly controlled
- immunosuppression
- evidence of mastoid, middle ear or skull base involvement
Suspected invasive or necrotising disease needs urgent ear, nose and throat assessment, microbiological sampling, imaging and specialist antimicrobial or antifungal planning. This is not a condition for self-treatment.
Practical advice for patients and expert patients
Patients can support recovery by protecting the ear canal while treatment is underway. Advice should be individualised by the treating clinician, but common measures include:
- keep the affected ear dry unless advised otherwise
- avoid swimming until cleared by a clinician
- do not use cotton buds or insert objects into the ear
- use prescribed drops exactly as directed
- attend follow-up if symptoms persist, because repeat cleaning may be needed
- tell the clinician about diabetes, immune problems, steroid use, biological therapies, chemotherapy, transplant medicines or previous ear surgery
- ask whether hearing aids, earmoulds or ear plugs need cleaning or review
- report severe pain, dizziness, facial weakness, worsening hearing loss or persistent discharge urgently
Important: online images of invasive aspergillosis can be frightening and often do not represent ordinary otomycosis. Most Aspergillus ear infections are local infections of the outer ear canal. The key is proper assessment, safe cleaning and appropriate treatment.
Frequently asked questions
Is Aspergillus otomycosis rare?
It depends on the setting. Otomycosis is common in some warm and humid regions but is less commonly recognised in many UK clinics. Aspergillus otomycosis may be unfamiliar to clinicians who do not often see fungal ear disease.
Is it the same as invasive aspergillosis?
Usually, no. Most Aspergillus otomycosis is a superficial infection of the outer ear canal. Invasive disease is rare but important, especially in people with diabetes, immunosuppression, severe pain or persistent infection.
Can an ear infection cause symptoms elsewhere in the body?
Otomycosis itself would not usually cause breathlessness, chest symptoms or systemic illness. If a person with suspected otomycosis is also breathless, has chest pain, fever, low oxygen levels or feels very unwell, those symptoms should be assessed separately and promptly.
Can it affect hearing?
Yes. Hearing may be reduced if the ear canal is blocked by fungal debris, discharge or swelling. Hearing often improves when the canal is cleaned and inflammation settles. Sudden hearing loss should be treated as a medical emergency and assessed urgently.
Should every case be cultured?
Not necessarily. Straightforward cases may be treated clinically. Culture and microscopy are more useful when symptoms are recurrent, severe, atypical, treatment-resistant, associated with perforation or surgery, or occur in an immunocompromised patient.
Are antifungal ear drops enough?
Often, topical treatment is effective, but drops may not work well if the ear canal is blocked with debris. Cleaning the canal is often as important as the antifungal medicine itself.
Can patients buy something and treat it themselves?
This is not recommended. Ear symptoms can have several causes, and some substances may be unsafe if the eardrum is perforated. Patients should seek clinical assessment before putting unprescribed antifungal, antiseptic, acidic, herbal or oil-based preparations into the ear.
Why does otomycosis come back?
Recurrence can happen if the canal remains damp, debris persists, the ear is repeatedly traumatised, a hearing aid mould traps moisture, eczema is present, antibiotics are repeatedly used, or an underlying condition such as diabetes or immune suppression is not recognised.
When to seek urgent medical help
Patients should seek urgent medical advice if they have:
- severe or worsening ear pain
- pain that wakes them at night
- swelling, redness or tenderness around the ear
- tenderness, swelling or redness over the mastoid bone behind the ear
- persistent discharge despite treatment
- sudden hearing loss or rapidly worsening hearing
- persistent, severe or worsening dizziness
- severe headache or vomiting
- facial weakness or changes in facial movement
- confusion, fever or feeling very unwell
- diabetes, immune suppression or recent chemotherapy or transplant treatment with ear infection symptoms
- previous ear surgery, grommets or known eardrum perforation with new discharge or pain
These symptoms do not prove invasive infection, but they should be assessed promptly.
Evidence gaps and uncertainty
The evidence base for otomycosis is improving but remains limited. Many studies are single-centre observational series from regions where otomycosis is more common. Treatment studies vary in diagnostic criteria, topical agents, follow-up duration and whether cleaning was standardised. There is no single universally accepted treatment regimen for all cases.
Important gaps include:
- limited high-quality randomised trials comparing topical antifungal treatments
- variable reporting of tympanic membrane status and previous ear surgery
- inconsistent use of fungal culture, molecular identification and susceptibility testing
- limited data on recurrence prevention
- limited evidence specific to UK practice
- uncertainty about the best systemic antifungal approach in rare invasive cases
For these reasons, this article should support but not replace specialist clinical judgement.
References
- Nazari T, Peymaeei F, Ghazi Mirsaid R, et al. Otomycosis: a systematic review and meta-analysis of prevalence and causative agents in the era of molecular diagnostics. BMC Infectious Diseases. 2025;25(1). doi: 10.1186/s12879-025-10954-y. PubMed
- Bojanović M, Stalević M, Arsić-Arsenijević V, et al. Etiology, Predisposing Factors, Clinical Features and Diagnostic Procedure of Otomycosis: A Literature Review. Journal of Fungi. 2023;9(6):662. doi: 10.3390/jof9060662. PubMed
- Wiegand S, Berner R, Schneider A, Lundershausen E, Dietz A. Otitis Externa: Investigation and Evidence-Based Treatment. Deutsches Ärzteblatt International. 2019. doi: 10.3238/arztebl.2019.0224. PubMed
- Koltsidopoulos P, Skoulakis C. Otomycosis With Tympanic Membrane Perforation: A Review of the Literature. Ear, Nose & Throat Journal. 2019;99(8):518–521. doi: 10.1177/0145561319851499. PubMed
- Mtibaa L, Halwani C, El Hamdi M, et al. A retrospective study of 43 cases of fungal malignant external otitis. Pan African Medical Journal. 2022;41. doi: 10.11604/pamj.2022.41.287.29585. PubMed
- Szigeti G, Sedaghati E, Mahmoudabadi AZ, et al. Species assignment and antifungal susceptibilities of black aspergilli recovered from otomycosis cases in Iran. Mycoses. 2011;55(4):333–338. doi: 10.1111/j.1439-0507.2011.02103.x. PubMed
- Jimenez-Garcia L, Celis-Aguilar E, Díaz-Pavón G, et al. Efficacy of topical clotrimazole vs. topical tolnaftate in the treatment of otomycosis: a randomized controlled clinical trial. Brazilian Journal of Otorhinolaryngology. 2020;86(3):300–307. doi: 10.1016/j.bjorl.2018.12.007. PubMed
- Mofatteh MR, Naseripour Yazdi Z, Yousefi M, et al. Comparison of the recovery rate of otomycosis using betadine and clotrimazole topical treatment. Brazilian Journal of Otorhinolaryngology. 2018;84(4):404–409. doi: 10.1016/j.bjorl.2017.04.004. PubMed
- Mao C, Li A, Hu J, et al. Efficient and accurate diagnosis of otomycosis using an ensemble deep-learning model. Frontiers in Molecular Biosciences. 2022;9:951432. doi: 10.3389/fmolb.2022.951432. PubMed
- Feng Y, Zhang Z, Fang W, et al. Profiling Drug Susceptibility and Species Identification of Aspergillus Isolates From Patients With Superficial Infection. Mycoses. 2025;68(4). doi: 10.1111/myc.70059. PubMed
- NICE Clinical Knowledge Summaries. Otitis externa. NICE CKS
Author and review information
Article type: Clinical and expert-patient evidence update
Intended audience: Ear, nose and throat clinicians, infectious diseases specialists, medical mycologists, general practitioners, specialist nurses, patients and carers seeking detailed information.
Last reviewed: June 2026
Review note: This article is for information and education. It should not replace assessment by a qualified clinician. Treatment choices depend on examination findings, tympanic membrane status, culture results where available, medical history, immune status and local prescribing guidance.
“`

Latest News posts
News archive