Browse information
Latest Articles
Support
For Professionals
Search
NAC & Guidance
Home
Archive by Category "NAC & Guidance"
NAC & Guidance
Speaking up about your healthcare: self-advocacy and independent advocacy
by GAtherton
Your Story Matters—but It Is Not Someone Else’s Future
by GAtherton
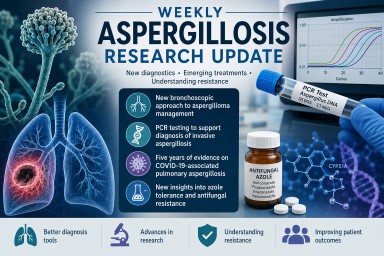
Weekly Aspergillosis Research Update: New Diagnostics, CAPA Evidence, and Why Azole Tolerance Matters
by GAtherton
About the National Aspergillosis Centre (NAC)
by GAtherton
Why the UK’s Infection Specialist Workforce Matters to People Living with Aspergillosis
by GAtherton
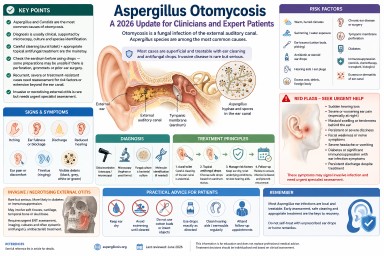
Aspergillus Otomycosis: A 2026 Update for Clinicians and Expert Patients
by GAtherton
More Than a Referral Centre: How the National Aspergillosis Centre Supports Patients and Healthcare Professionals Across the UK
by GAtherton
Professional Aspergillosis Update: May 2026
Audience: respiratory…
by GAtherton
The Power of Keeping a Health Diary When You Have Aspergillosis
by GAtherton
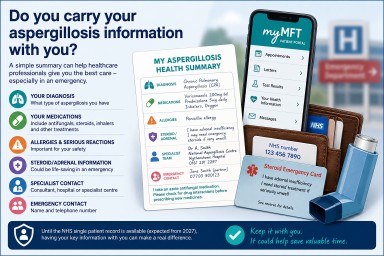
Do You Carry Your Aspergillosis Information With You?
by GAtherton
1
2
3
…
17