Browse information
Latest Articles
Support
For Professionals
Search
NAC & Guidance
Home
Archive by Category "NAC & Guidance"
(
Page 2
)
NAC & Guidance
What the UK Infection Workforce Report Means for Aspergillosis Patients and Specialists
by GAtherton
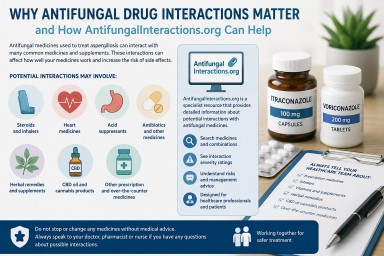
Why Antifungal Drug Interactions Matter — and How AntifungalInteractions.org Can Help
by GAtherton
Aspergillosis Trust: Supporting People Affected by Aspergillosis
by GAtherton
European Lung Foundation (ELF): Giving Patients a Voice in Respiratory Health
by GAtherton
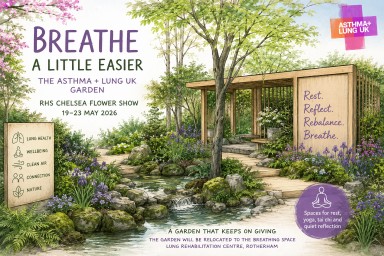
Breathe deeply at the Asthma + Lung UK Garden
by GAtherton
When Breathlessness Feels Severe — Even When Oxygen Levels Look “Normal”
by GAtherton
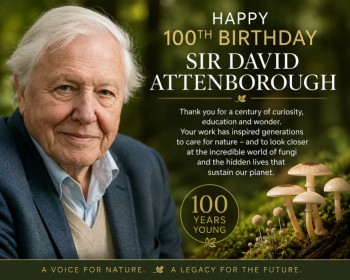
Sir David Attenborough at 100: Inspiring Wonder in Nature and Fungi
by GAtherton
Blue inhalers, combination inhalers and aspergillosis: what patients need to know
Recent news about “blue…
by GAtherton
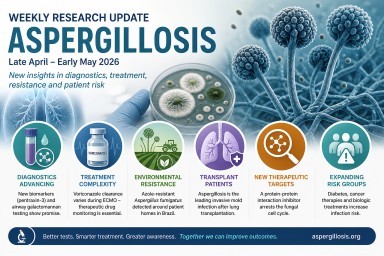
Weekly Aspergillosis Research Update April - May 2026
Search term: aspergillosis…
by GAtherton
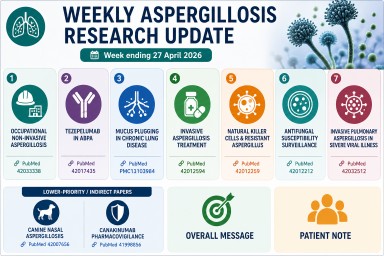
Weekly Aspergillosis Research Update: Week ending 27 April 2026
Highlights this week…
by GAtherton
1
2
3
4
…
17