NAC & Guidance
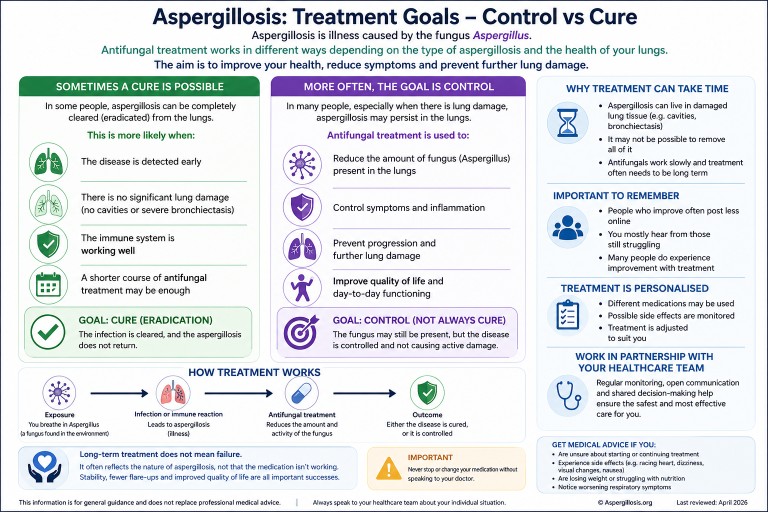
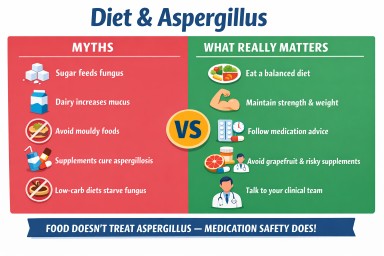
Can Aspergillosis Be Cured? Understanding Treatment, Control, and Long-Term Therapy
Last reviewed: April 2026…
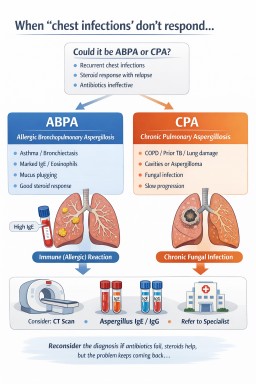
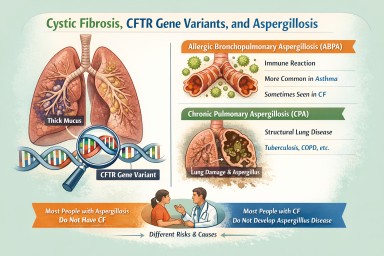
When ‘chest infections’ don’t respond: when to suspect ABPA or CPA (Clinical perspective)
Patients presenting with…


AntifungalInteractions.org – A Specialist Resource for Safer Antifungal Treatment
Last reviewed: April 2026…
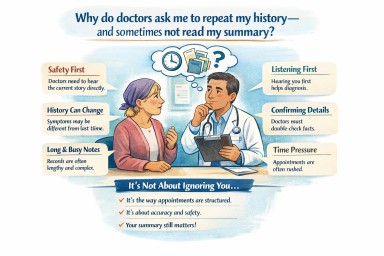
Why do doctors ask me to repeat my history — and sometimes not read my summary?
Last reviewed: 9 April 2026…