Key Shifts to Reinvent the NHS - The 10 Year plan
The plan introduces three radical shifts to modernize the NHS and secure its future:
-
🏥 Hospital → Community
-
Build a Neighbourhood Health Service: community health centres open 6 days/week for 12 hours/day
-
Provide integrated care closer to home—GPs, diagnostics, mental health, rehab, dentists, pharmacists, and even social support
-
Aim to reduce reliance on hospitals and cut waiting lists
-
-
📱 Analogue → Digital
-
Transform the NHS App into a “doctor in your pocket”—for appointments, advice, care plans, and self-referral
-
Embed AI to reduce admin, transcribe consultations, and support clinical decision-making
-
-
🛡️ Sickness → Prevention
-
Emphasize early intervention through more health checks, screenings, vaccines, and public health services
-
Shift funding towards community and preventative care, away from reactive hospital-based services
-
🏗 Underpinning Measures
To support these shifts, the plan introduces:
-
A new operating model & statutory framework to streamline the NHS structure
-
Transparency and accountability through metrics and patient feedback
-
Workforce transformation, including new training and wellbeing support
-
Innovation strategy harnessing genomics, AI, and tech
-
Financial reform via value-based funding—where providers are rewarded for outcomes
🔍 What This Means for You
-
Access to GP advice and care should be faster and more local – with reduced “8 am scramble”
-
More services like scans, mental healthcare, rehab, smoking cessation, and job support delivered at local centres
-
Greater convenience—use the App to manage care, book appointments, or message clinicians
-
Stronger focus on staying healthy—through screening, prevention, and early treatment support
🧩 Challenges & Expert Views
-
Funding & staffing: A £29 billion investment is pledged, but staffing shortages and infrastructure needs remain concerns
-
Implementation: Organisations like the King’s Fund highlight the absence of operational details and worry pilot projects may lead to regional variation
-
Behavioural shift: Success depends on NHS culture evolving—from reactive treatment to proactive, tech-enabled care
✍️ Final Take
The 10‑Year Health Plan represents a transformative vision: bring care closer to home, empower patients digitally, and focus on prevention. With strong backing from Starmer and Health Secretary Streeting, it aims to reshape NHS services by 2035. While optimism is growing, the effectiveness of implementation and securing resources will determine whether it truly delivers for patients and staff.
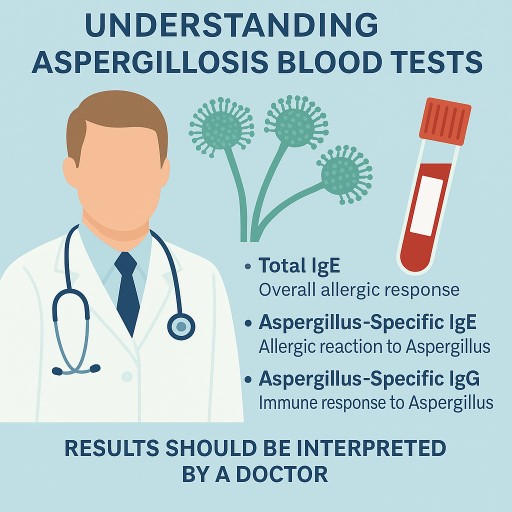
🧪 Understanding Aspergillosis Blood Tests: IgE and IgG Explained
For patients in the UK and internationally
If you are living with aspergillosis, including forms such as chronic pulmonary aspergillosis (CPA), allergic bronchopulmonary aspergillosis (ABPA), or severe asthma with fungal sensitisation (SAFS), you may have had blood tests that measure how your immune system responds to Aspergillus, a common type of fungus.
This guide explains the role of these tests, why results may vary between hospitals, and what they mean for diagnosis and ongoing care.
🔬 What Are These Blood Tests?
✅ Total IgE
-
Measures your body’s overall allergic response.
-
Often raised in people with ABPA or SAFS, but also in asthma, eczema, and parasitic infections.
✅ Aspergillus-Specific IgE
-
Detects allergic reaction specifically to Aspergillus fumigatus.
-
Helps diagnose ABPA and SAFS.
✅ Aspergillus-Specific IgG
-
Measures immune response to longer-term exposure to Aspergillus.
-
Mainly used to help diagnose CPA, but can also support ABPA diagnosis.
📊 What Are the Normal Ranges?
📌 Total IgE Reference Ranges (UK Examples)
| Age Group | NHS Reference Range |
|---|---|
| Children | Varies by age, up to ~75 kU/L |
| Adults | 0–75 to 5–120 kU/L (depends on hospital) |
In ABPA, total IgE is usually > 500 kU/L, and sometimes exceeds 1000 kU/L.
📌 Aspergillus-Specific IgE: Positive Ranges
| Level (kUA/L) | What It Means |
|---|---|
| <0.35 | Negative |
| 0.35–0.7 | Borderline |
| 0.7–3.5 | Positive |
| >3.5 | Strongly positive |
| >17.5 | Very strongly positive |
📌 Aspergillus-Specific IgG: Positive Ranges
| Test Used | Positive Threshold |
|---|---|
| ImmunoCAP (most NHS labs) | >27–40 mgA/L |
| Bordier ELISA | >50–75 AU/mL |
| LDBio ICT (lateral flow strip) | Visual positive line |
The exact “positive” level depends on the test platform used by the lab. Always check which test was used when reviewing results.
🧪 Why Do Reference Ranges Differ Between Hospitals?
It’s common for different hospitals and countries to use slightly different tests and reference ranges. This is due to:
-
Different brands or types of test kits (e.g. ImmunoCAP, Bordier, Serion, LDBio)
-
Varying units of measurement
-
Locally validated ranges based on the population
-
Differences in clinical protocols or disease thresholds
For example, a test result of Aspergillus IgG at 38 mgA/L may be seen as positive in one hospital and borderline in another depending on which assay is used.
🧭 How These Tests Fit into Aspergillosis Diagnosis
🩺 Blood Tests Help Guide the Diagnosis, But Are Not Enough Alone
| Condition | Typical Test Findings |
|---|---|
| ABPA | Total IgE >500 kU/L + Aspergillus-specific IgE >0.35 kUA/L + often raised IgG |
| SAFS | Raised Aspergillus-specific IgE + asthma + poor steroid response |
| CPA | Aspergillus-specific IgG essential; total IgE and IgE may be normal |
Diagnosis always depends on a combination of factors — not just a blood test.
🧩 Other Essential Parts of Diagnosis
| Diagnostic Tool | What It Does |
|---|---|
| Chest CT scan | Detects cavities, nodules, or bronchiectasis |
| Sputum culture or PCR | Confirms presence of Aspergillus |
| Galactomannan or beta-D-glucan | Sometimes used to monitor invasive disease |
| Lung function tests | Assess asthma or airflow limitation |
| Symptoms | Breathlessness, cough, weight loss, fatigue |
| Treatment response | Helps confirm diagnosis if patient improves with treatment |
Blood tests are just one piece of the puzzle. Doctors always interpret them alongside imaging, symptoms, and history.
🩺 What About Management?
Once diagnosed, managing aspergillosis involves more than just monitoring blood tests. Your care plan may include:
-
Antifungal medication (e.g. itraconazole, voriconazole)
-
Steroids or biologics (especially in ABPA)
-
Physiotherapy to clear mucus
-
Regular imaging (e.g. CT scans)
-
Monitoring IgE/IgG over time
-
Patient support for fatigue, emotional health, and quality of life
📋 Understanding Your Results: What Do They Mean?
When you receive blood test results like total IgE, Aspergillus-specific IgE, or Aspergillus-specific IgG, you may see a number alongside a reference range (sometimes called the “normal range”). This helps show whether your result is considered low, normal, or high in that specific laboratory.
🧾 Example:
| Test | Your Result | Lab Reference Range | Interpretation |
|---|---|---|---|
| Total IgE | 580 kU/L | 0–120 kU/L | Elevated |
| Aspergillus-specific IgE | 0.9 kUA/L | >0.35 = positive | Positive |
| Aspergillus-specific IgG | 39 mgA/L | 0–27 mgA/L | Borderline high |
❓ Is a Slightly High Result a Problem?
-
A mild or borderline elevation does not automatically mean disease.
-
Some people may have a raised IgE or IgG but no active symptoms or signs of aspergillosis.
-
Other people with clear disease may have only modest rises in their test levels.
🔍 Important: Test results must always be interpreted in the context of your overall health, scan results, and symptoms.
✅ Let Your Doctor Guide You
It’s completely normal to feel uncertain or anxious about test results — especially if a number is just above the “normal range.” But:
-
Let your doctor or specialist interpret the result as part of your whole clinical picture.
-
They may repeat the test, combine it with a CT scan or lung function test, or monitor changes over time.
-
Some test levels, like total IgE in ABPA, are tracked over months to see if treatment is working.
💬 Ask your doctor:
“How does this result fit in with my symptoms and scan findings?”
🧠 Final Takeaway
Blood tests like IgE and IgG are essential tools in diagnosing and managing aspergillosis, but they are only one part of the bigger picture. Imaging, symptoms, response to treatment, and even how you feel day-to-day are just as important.
Always ask for a copy of your results with reference ranges, and bring them to appointments.
And remember — a slightly raised result doesn’t always mean something is wrong. Your doctor is the best person to interpret it for you.
🌫️ A Life Shaped by Mould: One Person’s Journey with CPA and Lung Disease
Sadly, at the time of writing this story has to be paid for to read the full article. What follows is a summary of the free-to-access abstract.
“It started with damp walls – but it didn’t end there.”
This is the story of someone who spent a lifetime battling the hidden effects of mould exposure and fungal lung disease, from childhood through adulthood. Their experience is a powerful reminder of how long-term exposure to poor indoor environments — especially damp, flood-prone homes — can leave a lasting imprint on lung health.
🧒 Early Clues: Breathing Problems in Childhood
-
The author grew up in mouldy homes, regularly affected by floods.
-
As a teenager, they suffered from collapsed lungs, underwent pleurectomies, and were diagnosed with blebs (small air-filled sacs on the lung lining).
-
No one realised at the time that this could be linked to inhaled fungal spores.
🩺 The Long Road to Diagnosis
-
Years later, symptoms returned: chest infections, breathlessness, persistent coughing.
-
Eventually, doctors diagnosed:
-
Chronic pulmonary aspergillosis (CPA) – a long-term fungal infection
-
Severe bronchiectasis – a condition where the airways become damaged and inflamed
-
The root cause was now clear: years of breathing in airborne mould spores had likely caused permanent lung damage.
💊 Managing CPA: A Complex Balancing Act
The chapter describes the difficulty of living with CPA, including:
-
Strong antifungal medications (like itraconazole or posaconazole) and their side effects
-
Emergency lung procedures
-
Ongoing adjustments in daily life — from avoiding certain environments to managing fatigue
🤝 What Helped Most: Self-Advocacy and Support
This is also a story of resilience and empowerment. The author learned to:
-
Ask better questions at medical appointments
-
Work closely with specialists in fungal lung disease
-
Use trusted online resources to understand their condition
-
Keep going, even when progress was slow
💬 “I had to become my own advocate – not to fight my doctors, but to work with them more effectively.”
🧭 Advice for Others
The author shares practical tips that could help anyone dealing with CPA, bronchiectasis, or long-term lung illness:
-
Track your symptoms and treatments
-
Stay informed – but avoid misinformation online
-
Get help from respiratory physiotherapists
-
Don’t ignore your environment – especially damp, mouldy places
-
Keep asking questions until the answers make sense
🌟 A Message of Hope
This chapter isn’t just a medical account – it’s a message of hope and strength. It shows how understanding your own health, building a good medical team, and staying proactive can make a big difference, even in the face of serious illness.

Taking Charge: How to Get Involved in Decisions About Your Treatment
When you live with a long-term condition like aspergillosis, ABPA, CPA, or severe asthma, you may face tough decisions about medication, side effects, and quality of life. Treatments like biologics can offer huge benefits—but they also carry risks, and no one knows your body, lifestyle, or priorities better than you do.
The NHS is clear in its long-term plan: you should be involved in every major decision about your care. This is known as shared decision-making (SDM), and it means clinicians and patients working together to make the best choices—not just being told what to do.
Here’s how you can become more confident in taking part in your own care—and how to help your clinical team include you.
🪜 Step-by-Step: How to Join the Decision-Making Process
✅ 1. Know You Have a Right to Be Involved
You are not being "difficult" by asking questions or wanting to be part of the decision. The NHS encourages shared decision-making—and it’s your health.
🗣 “I’d like to understand the options and be involved in deciding what’s best for me.”
✅ 2. Ask for the Options – Including None
Sometimes we are only offered one treatment, but most decisions have at least 2 or 3 choices. For example:
-
Start or delay biologics?
-
Try antifungals again or monitor symptoms?
-
Continue with current care or make a change?
Ask:
🗣 “What are my options, including the option of not doing anything right now?”
✅ 3. Talk About What Matters Most to You
Doctors often focus on test results or scan findings. But you may be more concerned about fatigue, side effects, work, travel, or caring for family.
Let them know what your priorities are:
🗣 “My top goal is to stay out of hospital and manage breathlessness so I can keep working.”
🗣 “I can live with minor side effects, but I don’t want something that weakens my immune system too much.”
✅ 4. Understand the Risks and Benefits
Every treatment, including biologics, is a balance—they reduce inflammation but may make you more vulnerable to infection. That doesn’t mean you shouldn’t take them, but it’s important to understand the trade-offs.
Ask:
🗣 “What are the likely benefits of this treatment for someone like me? What are the possible side effects?”
🗣 “How will this affect my overall health and day-to-day life?”
✅ 5. Ask for Time to Reflect
You don’t need to make big decisions in a 10-minute appointment.
🗣 “Can I take this information home and think about it? I’d like to talk with family or other patients before I decide.”
It’s okay to not decide straight away.
✅ 6. Keep Track of Questions and Progress
Write things down before your appointment. You can even bring someone with you, or ask to record the discussion on your phone.
Apps and treatment diaries help you track side effects, symptoms, and goals, so you and your team can review how well things are working later.
✅ 7. Use Supportive Tools and People
Ask for:
-
Leaflets, videos, or trusted websites to read later
-
A follow-up call with a specialist nurse
You could say:
🗣 “Can you recommend a trusted place to read more about this? I’d like to understand it in my own time.”
🧠 A Shift in Thinking: It’s Not About a Quick Fix
We’ve all grown up with advertising that tells us “This treatment will fix the problem.” But in reality, every treatment is a trade-off—between the benefits it brings and the side effects or limitations it may cause.
Even doctors can fall into the trap of focusing only on what they can treat in their specialty—lungs, infections, skin—and miss how treatments affect the whole person.
You can help by:
-
Gently reminding them of the bigger picture
-
Asking them to explain in plain language
-
Saying honestly how things are affecting your life, not just your lungs
🌈 Your Quality of Life Is the Priority
In the end, what matters is how you feel and function. For some, a small side effect might be worth the gain in lung function or fewer flare-ups. For others, it may not. Only you can make that call—with the right information and support.
📌 Good care means making decisions with you, not for you.
📥 Want to Take This Further?
Ask your clinic or GP about:
-
Shared Decision-Making tools (they’re part of NICE guidelines)
-
Getting written summaries of discussions and next steps
And remember: you’re not just a patient—you’re a partner in your care.
Best Types of Cleaning Products for Chemical Sensitivities
For people with chemical sensitivities—such as Multiple Chemical Sensitivity (MCS), asthma, or other respiratory conditions—it's important to use gentle, non-toxic cleaning products that don't contain harsh chemicals, fragrances, or volatile organic compounds (VOCs). Here's an overview:
✅ Best Types of Cleaning Products for Chemical Sensitivities
🧴 1. Fragrance-Free and Dye-Free Products
-
Look for labels that say “fragrance-free,” “unscented,” and “free and clear.”
-
Avoid products labeled "natural" if they still contain essential oils or botanical fragrances (these can still trigger reactions).
🌿 2. Simple, Non-toxic Ingredients
Safer cleaning agents often include:
-
White vinegar – natural disinfectant, but avoid if the smell is bothersome.
-
Baking soda – gentle abrasive cleaner, excellent for scrubbing.
-
Castile soap – a mild, vegetable-based soap (e.g. Dr. Bronner’s).
-
Hydrogen peroxide (3%) – for disinfecting and stain removal.
-
Rubbing alcohol (70%) – effective on surfaces, but test for sensitivity.
🔄 3. DIY Cleaning Solutions
Many people with sensitivities prefer to make their own:
-
All-purpose cleaner: 1 part vinegar + 1 part water (optional: a drop of castile soap).
-
Glass cleaner: 2 cups water + 2 tablespoons vinegar + 1 tablespoon rubbing alcohol.
-
Soft scrub: Baking soda + a small amount of water or castile soap.
👩⚕️ Recommendations from Support Groups and Allergy Specialists
-
Choose products that are certified by:
-
EcoLogo
-
Green Seal
-
Safer Choice (US EPA)
-
Allergy UK’s Seal of Approval
-
-
Common brands used by sensitive individuals:
-
Ecover Zero
-
Attitude (Sensitive line)
-
Seventh Generation Free & Clear
-
Molly’s Suds
-
Clean Living
-
Simple Truth Free & Clear
-
(Always patch test new products first.)
🧠 Tips from People Living with Sensitivities
-
Ventilate well during and after cleaning.
-
Use microfiber cloths and steam mops to reduce the need for chemical cleaners.
-
Avoid air fresheners, candles, and essential oils, even if labeled “natural.”
-
Store cleaning products away from living spaces to limit fumes.

🌡️ How to Store Your Medicines Safely in Hot Weather
Many prescription medicines must be stored below 25°C to remain safe and effective. During summer or heatwaves, especially when temperatures rise above 30°C, you need to take extra care.
This guide explains what to do to keep your medicines safe at home or while travelling.
❓ Why It Matters
Medicines exposed to too much heat can:
-
Lose effectiveness
-
Change in appearance or texture
-
Become unsafe to use
This is especially true for:
-
Antibiotics
-
Inhalers
-
Liquid medicines
-
Hormone tablets (e.g. thyroxine)
-
Biologics or injectables (some require refrigeration)
📦 What "Store Below 25°C" Means
-
This refers to room temperature – ideally between 15°C and 25°C.
-
Some medicines may tolerate brief periods above 25°C, but prolonged heat can degrade them.
-
Do not refrigerate medicines unless specifically instructed – cold can also damage some drugs.
🏠 At Home: Tips for Keeping Medicines Cool
| ✅ Do | ❌ Avoid |
|---|---|
| Store in a cool, dark place | Windowsills or near radiators |
| Use a shaded cupboard or wardrobe | Kitchen cupboards near ovens |
| Consider an insulated box (without ice) | Bathrooms (can get hot and humid) |
| Monitor the temperature with a small digital thermometer | Leaving in direct sunlight |
You can buy inexpensive thermometers online to check storage temperatures.
🌞 In a Heatwave
If indoor temperatures go above 25°C for more than a few hours:
-
Move medicines to the coolest part of your home (e.g. north-facing room or basement).
-
Close blinds and curtains during the day to keep rooms cooler.
-
Use fans or portable air conditioners if available.
-
Keep medicines away from heat-generating electronics.
✈️ Travelling or on Holiday
-
Never leave medicine in a hot car, especially glove boxes or boots.
-
Use a cool bag, insulated travel pouch, or medication wallet with a cooling gel pack.
-
In hotels, store medicines in a shaded cupboard or the fridge only if the label allows it.
-
Avoid storing medicines in your luggage if it may be left in the sun or overheated.
✅ Signs Your Medicine May Be Affected
Contact your pharmacist if:
-
The medicine looks or smells different
-
Tablets have melted, crumbled or discoloured
-
Liquids have separated or changed consistency
-
You’re unsure whether the medicine has been exposed to prolonged heat
🗨️ What the NHS and UK Pharmacists Say
-
Short-term exposure to temperatures slightly above 25°C is usually not harmful.
-
Medicines stored above 25°C for several days may need to be replaced – ask your pharmacist.
-
Pharmacies use temperature-controlled storage and monitor heat during hot weather – you can do the same at home.
Sources include NHS Trusts, SPS (Specialist Pharmacy Service), and Royal Pharmaceutical Society guidance.
📋 Quick Tips Checklist
✅ Keep medicines in their original packaging
✅ Avoid windowsills, kitchens, and bathrooms
✅ Use a shaded, cool cupboard or wardrobe
✅ Monitor room temperatures during heatwaves
✅ Carry medicines in a cool bag when travelling
✅ Check for changes in medicine appearance
✅ Ask a pharmacist if in doubt
📞 Need advice?
Speak to your pharmacist or GP if you're unsure whether a medicine has been affected by heat or if it still seems safe to use.

Research Outcomes Explained: 2025
Over the years, a growing number of research studies have been published by leading experts in chronic aspergillosis—including CPA (chronic pulmonary aspergillosis), ABPA (allergic bronchopulmonary aspergillosis), SAFS (severe asthma with fungal sensitisation), and related conditions—in the UK and around the world.
Below you’ll find summaries of studies published so far in 2025, including versions written in plain language to help patients better understand what the findings might mean for them.
Several of these studies were conducted in the UK, with the National Aspergillosis Centre (NAC) and the University of Manchester acting as key research hubs. If you’ve taken part in aspergillosis-related research in the past—perhaps even several years ago—you may have contributed to some of these studies.
To learn more about each study and where the research was carried out, click on the links provided. These will take you to a summary page with full details, including a PubMed link to the original publication.
1. Stem Cell Transplant in STAT3-HIES: What It Means for Aspergillosis Patients
2. Understanding Immune Problems in CPA: What Recent Research Reveals
3. CPA After Tuberculosis: What a New Study from Indonesia Tells Us
4. Chronic Pulmonary Aspergillosis (CPA) and Mortality: Key Findings from a Major Review
5. New Hope for Drug-Resistant Aspergillosis: A Closer Look at a Promising Antifungal Peptide
6. Aspergillus terreus in the Environment: What Patients Should Know
7. Can Blood Tests Help Diagnose and Monitor ABPA?
8. Aspergillosis in Dolphins and Whales: What It Tells Us About the Environment
9. Understanding Drug Interactions with Isavuconazole (Cresemba)
10. New Hope for Difficult Fungal Infections: Olorofim
11. When NTM and Aspergillosis Occur Together: What This Study Found
12. Bronchial Artery Embolisation: What Patients Should Know
13. Aspergillus Lung Infections: What This Study Found in a Major French Hospital
14. How Does CPA Affect People with HIV?
15. How the Immune System Responds in Chronic Pulmonary Aspergillosis (CPA)
16. What Can a CT Scan Tell Us About CPA?
1. Stem Cell Transplant in STAT3-HIES: What It Means for Aspergillosis Patients
The published paper is entitled "Allogeneic haematopoietic stem cell transplantation for STAT3 hyper-IgE syndrome: a worldwide study" and you can read it here (Pubmed).
Some people living with aspergillosis (a fungal lung infection) may also have an underlying immune condition called STAT3 hyper-IgE syndrome, or STAT3-HIES for short. This is a rare inherited condition that affects both the immune system and other parts of the body.
🧬 What is STAT3-HIES?
STAT3-HIES (Signal Transducer and Activator of Transcription 3 – Hyper Immunoglobulin E Syndrome) is a genetic disorder that causes:
-
Frequent skin and lung infections
-
Long-term lung damage such as:
-
Bronchiectasis (widened airways that trap mucus and cause infections)
-
Pneumatoceles (air-filled cysts in the lungs)
-
-
Fungal lung infections such as aspergillosis
-
Other complications, such as:
-
Lymphoma (a cancer of the immune system)
-
Bone fractures
-
Vasculopathy (blood vessel damage)
-
This condition occurs because of a mutation in the STAT3 gene, which affects how the immune system responds to infections.
🧪 What is HSCT?
HSCT stands for Haematopoietic Stem Cell Transplantation. It is a treatment where faulty immune cells are replaced with healthy cells from a donor. These new stem cells can rebuild a working immune system and help prevent infections.
Doctors may recommend HSCT in severe cases of STAT3-HIES, especially when infections are frequent or serious, or if lymphoma develops.
🧾 What Did the Study Look At?
An international team of doctors studied 41 patients with STAT3-HIES from across the world who received HSCT over a period of 28 years. Here's what they found:
-
93% of patients had the transplant because of serious infections.
-
7% had HSCT due to lymphoma.
-
Patients were aged 4 to 45 years, with an average age of 14 at the time of transplant.
-
Most patients had lung disease before the transplant:
-
93% had chronic respiratory issues
-
68% had lung tissue damage (parenchymal disease)
-
32% had previous fungal lung infections, including aspergillosis
-
💉 How Was the Transplant Done?
-
Patients received stem cells from either blood or bone marrow.
-
Donors included:
-
MUD: Matched Unrelated Donor (44%)
-
MFD: Matched Family Donor (44%)
-
MMFD: Mismatched Family Donor (10%)
-
One patient had a MMUD: Mismatched Unrelated Donor (9 out of 10 matched)
-
-
Conditioning treatment (chemotherapy to prepare for transplant) included:
-
Treosulfan-based regimens (used in 59% of patients)
-
Busulfan-based regimens (24%)
-
Melphalan-based regimens (17%)
-
Some regimens also included thiotepa.
-
📈 What Were the Results?
-
Overall Survival (OS) at 5 years was 93%
-
OS = percentage of patients still alive
-
-
Event-Free Survival (EFS) at 5 years was 90%
-
EFS = no major complications like death, transplant failure, or chronic rejection
-
-
Acute Graft-versus-Host Disease (GvHD) occurred in 22% (moderate to severe cases)
-
GvHD = when the donor’s immune cells attack the patient’s body
-
-
Infections improved:
-
87% of patients had fewer or no lung infections after transplant
-
-
However, 20% of patients developed new bone fractures after transplant
🩺 What Does This Mean for Patients?
For patients with STAT3-HIES who suffer from repeated infections, including aspergillosis, HSCT can be a life-changing treatment. It:
-
Helps rebuild the immune system
-
Reduces serious lung and skin infections
-
Allows many patients to live healthier lives
However:
-
The transplant may not improve all other complications, such as bone weakness or blood vessel issues.
-
Some patients will still need follow-up care for these problems.
📣 In Summary
-
STAT3-HIES is a rare immune condition that can cause serious lung infections, including aspergillosis.
-
HSCT (stem cell transplant) offers new hope, especially for young people with repeated infections or complications like lymphoma.
-
This international study shows that even patients with severe lung problems can do well after transplant, with a high survival rate and fewer infections.
-
Some complications (like fractures) may still occur, so long-term care is still important.
If you or someone you know is affected by STAT3-HIES or aspergillosis, speak to your clinical team about the options available — including whether HSCT might be a possibility, and what support is available before and after treatment.
2. 🦠 Understanding Immune Problems in CPA: What Recent Research Reveals
A study exploring why some people's immune systems struggle to control CPA
The published paper is entitled "Dendritic cell dysfunction, including impaired IL-12 production, is associated with chronic pulmonary aspergillosis" and you can read it here (Pubmed).
What is CPA?
Chronic Pulmonary Aspergillosis (CPA) is a long-term fungal lung infection caused by Aspergillus, a common mould. People with damaged lungs—often from conditions like bronchiectasis or previous tuberculosis (TB)—can be more vulnerable to CPA.
Although CPA is known to cause ongoing cough, breathlessness, fatigue, and weight loss, researchers are still learning why some people’s immune systems fail to control the fungus.
🔬 What Did the Study Look At?
This research compared the immune systems of:
-
25 people with CPA
-
25 people with bronchiectasis but no fungal infection
Researchers took blood samples from both groups and looked closely at the immune cells using flow cytometry (a lab technique for studying cell types and how active they are).
They studied immune cells at rest, and also after exposing them to a substance called Zymosan, which mimics fungal infection. This helps test how well immune cells respond to fungal threats.
🧪 What Did They Find?
Here’s what the researchers discovered about people with CPA:
1. More Neutrophils
-
CPA patients had higher levels of neutrophils, a type of white blood cell involved in fighting infection.
-
This may reflect ongoing inflammation.
2. Weaker Dendritic Cell Response
-
CPA patients had fewer dendritic cells (DCs), especially the type called cDC1s.
-
Dendritic cells act like “messengers” of the immune system – alerting and activating other cells.
3. Poor Activation After Challenge
-
When the immune cells were exposed to Zymosan, CPA patients’ dendritic cells and monocytes responded less effectively.
-
These cells showed reduced activity markers, especially:
-
IL-12p40 and TNFα (important for starting immune responses)
-
CD86 (helps activate other immune cells)
-
4. IFNγ Pathway May Be Affected
-
IL-12 normally helps trigger interferon gamma (IFNγ), a key molecule for fighting fungal infections.
-
Lower IL-12 suggests CPA patients may not produce enough IFNγ, weakening their ability to control the fungus.
5. Interesting Role of Tuberculosis History
-
CPA patients who had previous TB showed more activated dendritic cells.
-
This might reflect some form of “innate immune memory” – where past infections affect future immune responses.
🤖 What Else Did They Do?
The team also used machine learning (a type of computer analysis) to check if immune cell patterns could help predict who has CPA.
✅ They found that these immune differences were strong enough to separate CPA patients from those with bronchiectasis alone.
🩺 Why This Matters for Patients
-
This study gives important clues about how CPA affects the immune system — especially the early "alert" phase when the body first recognises fungi.
-
Understanding these changes could lead to better diagnostic tools, and even new treatments that help “retrain” the immune system.
-
It also shows that past lung infections like TB can change how the immune system works in lasting ways.
📌 In Summary
-
CPA patients have immune dysfunction that affects dendritic cells and monocytes.
-
These problems may cause reduced IFNγ production, a key defence against fungal infections.
-
People with a history of TB may have a different immune pattern that could affect CPA progression.
-
This study helps explain why some people develop CPA while others don’t, even if both have damaged lungs.
If you have CPA and a history of TB or are struggling with repeated infections, this research may help your doctors understand more about your condition — and how to manage it better in future.
3. 🦠 CPA After Tuberculosis: What a New Study from Indonesia Tells Us
Understanding CPA in people who’ve had TB and still have lung symptoms
The published paper is entitled "A Silent Threat in Post-Tuberculosis Patients: Chronic Pulmonary Aspergillosis Survey in Multiple Regions of Indonesia (I-CHROME Study)" and you can read it here (Pubmed).
🔍 Why Was This Study Done?
Many people who have had tuberculosis (TB) are left with long-term damage in their lungs — such as cavities (holes in the lung tissue). These damaged areas can become infected with a fungus called Aspergillus, leading to a condition called chronic pulmonary aspergillosis (CPA).
This study looked at how common CPA is in people in Indonesia who have recovered from TB but still have lung symptoms and cavities. Researchers also looked at which tests helped diagnose CPA and whether it differed by region.
👥 Who Was Studied?
-
219 people with a history of TB and ongoing respiratory symptoms
-
All had lung cavities seen on chest scans
-
They were divided into:
-
144 patients with CPA
-
75 patients without CPA
-
🧪 How Was CPA Diagnosed?
Doctors used international guidelines to diagnose CPA, combining:
-
Symptoms (like ongoing cough)
-
Lung scans (X-ray or CT scan)
-
Tests for the fungus Aspergillus:
-
Blood tests for Aspergillus-specific IgG antibodies using:
-
ICT (Immunochromatographic test)
-
ELISA (Enzyme-linked immunosorbent assay)
-
-
Sputum fungal cultures to try to grow the fungus from mucus
-
📈 What Did They Find?
🫁 Symptoms and Lung Damage
-
Persistent cough was much more common in people with CPA (83%)
-
Lung scan findings like cavities and fibrosis (scarring) were strongly linked to CPA
🧬 Blood Tests Work Better Than Sputum Culture
-
Aspergillus-specific IgG antibodies were a reliable indicator of CPA:
-
69% tested positive using ICT
-
63% tested positive using ELISA
-
-
However, growing the fungus from sputum (culture) was not a reliable way to confirm CPA on its own
🌍 Differences by Region
-
CPA was more common in Region 1 (75%) than in Region 2 (56%)
-
The most common fungi found were:
-
Aspergillus fumigatus
-
Aspergillus niger
-
🩺 Why Is This Important?
-
People with past TB and persistent lung symptoms may be at high risk of CPA, especially in regions with poor access to advanced medical care.
-
Cough, cavities on scans, and blood tests for Aspergillus IgG are important tools to help diagnose CPA.
-
Testing mucus (sputum) for the fungus is less useful on its own.
-
Regional differences in CPA rates suggest that local strategies are needed to improve diagnosis and care.
📌 What This Means for Patients
If you have had TB in the past and now have a chronic cough, lung cavities, or ongoing symptoms, ask your doctor about:
-
Blood tests for Aspergillus IgG
-
A CT scan to check for cavities and scarring
-
Whether CPA might be causing your symptoms
Getting the right diagnosis is key — CPA is treatable, but often missed unless specifically looked for.
4. Chronic Pulmonary Aspergillosis (CPA) and Mortality: Key Findings from a Major Review
Background
Chronic Pulmonary Aspergillosis (CPA) is a long-term fungal infection of the lungs that remains difficult to treat and is linked to significant illness and death. Researchers conducted a systematic review and meta-analysis of global studies to understand how often CPA leads to death and what factors make poor outcomes more likely.
The published paper is entitled "Mortality in chronic pulmonary aspergillosis: a systematic review and individual patient data meta-analysis" and you can read it here (Pubmed).
Study Methods
-
Researchers reviewed studies from PubMed, Scopus, Embase, and Web of Science from inception to August 15, 2023.
-
They included 79 studies (8778 patients) in the pooled mortality analysis and 15 studies (1859 patients) with detailed individual patient data.
-
The focus was on 1-year and 5-year mortality, patient demographics, underlying lung diseases, treatment type, and CPA subtypes.
-
Analysis included both summary data and individual patient data (IPD), using advanced statistical techniques (e.g., Cox proportional hazards model).
Key Findings
📊 Mortality Rates
-
Overall CPA mortality: 27% (range 22–32%)
-
1-year mortality: 15% (range 11–19%)
-
5-year mortality: 32% (range 25–39%)
🫁 Effect of Underlying Lung Disease
-
CPA with pulmonary tuberculosis: 25% mortality
-
CPA with chronic obstructive pulmonary disease (COPD): 35% mortality
-
CPA patients who had surgical treatment had much lower mortality: 3%
⚠️ Factors That Increase Risk of Death
-
Older age: Risk increases by 25% with each additional decade of age.
-
CPA subtype:
-
Chronic cavitary CPA and subacute invasive aspergillosis carried higher mortality.
-
Simple aspergilloma had the lowest mortality.
-
-
Comorbidities:
-
Patients with underlying malignancy had significantly worse outcomes.
-
A history of tuberculosis had relatively better outcomes.
-
Conclusion
CPA is a serious and life-threatening condition, particularly for older adults and those with complex forms of the disease or multiple underlying health conditions. Despite treatment, death rates remain high — especially at 5 years.
Clinical and Patient Implications
-
Risk stratification is crucial: not all patients with CPA have the same risk.
-
CPA should be treated early and aggressively in high-risk patients.
-
Surgical options may be considered in selected cases.
-
Better long-term care pathways and tailored treatment approaches are needed.
Next Steps for Research
The authors urge future studies to:
-
Focus on CPA subtypes and tailored treatment strategies.
-
Improve risk-based management.
-
Study outcomes in low-resource settings, where TB and CPA commonly overlap
5. 🧪 New Hope for Drug-Resistant Aspergillosis: A Closer Look at a Promising Antifungal Peptide
The published paper is entitled "Solid-state NMR Reveals Reorganization of the Aspergillus fumigatus Cell Wall Due to a Host-Defence Peptide" and you can read it here (Pubmed).
⚠️ The Problem
Treating aspergillosis — especially drug-resistant strains of Aspergillus fumigatus — is becoming increasingly difficult.
-
There are only a few antifungal medicines available today.
-
Some strains of Aspergillus fumigatus are becoming resistant to these medicines, especially azoles, the most commonly used type.
This means that new treatments are urgently needed.
🧬 A New Discovery: The Power of Cathelicidin-2
Scientists are studying a natural substance called cathelicidin-2, part of the body’s immune system (a “host defence peptide”).
Early research shows that cathelicidin-2 can slow down or stop the growth of drug-resistant Aspergillus fumigatus.
But until now, researchers didn’t fully understand how it works.
🔬 What Did This Study Find?
Using advanced imaging techniques, researchers closely studied how cathelicidin-2 interacts with the fungal cell wall – the protective outer layer of the fungus.
Here’s what they found:
-
Cathelicidin-2 targets key parts of the fungal cell wall, especially a substance called galactosaminogalactan, which helps the fungus cause disease.
-
It also affects other sugars and proteins in the cell wall.
-
After longer exposure, the peptide allows more water to enter the tough outer cell wall, making it easier for it to reach the fungus’s inner membrane — where it may be able to kill the fungus.
💡 Why This Matters for Patients
This study:
-
Helps scientists understand how to attack drug-resistant Aspergillus more effectively.
-
Could lead to the development of new antifungal treatments, based on how cathelicidin-2 works.
-
Offers new hope for patients who can’t tolerate existing antifungal drugs or whose infections are no longer responding to treatment.
🩺 What’s Next?
This is still early-stage research, and cathelicidin-2 is not yet available as a medicine. But understanding how it works is a big step toward designing better, safer antifungal drugs for the future.
If you have concerns about antifungal resistance or treatment options, speak to your specialist team or ask about ongoing research and clinical trials.
6. 🌍 Aspergillus terreus in the Environment: What Patients Should Know
The published paper is entitled "Exploring Factors Driving the Uneven Distribution of Aspergillus terreus in an Austrian Hotspot Region" and you can read it here (Pubmed).
A closer look at a hard-to-treat Aspergillus species found in Austrian soil
🦠 What is Aspergillus terreus?
Aspergillus terreus is a type of fungus that can cause aspergillosis, a serious lung condition. Like other Aspergillus species, it lives in the environment (especially in soil), but A. terreus presents some unique challenges:
-
It can spread throughout the body (dissemination) in vulnerable patients.
-
It often does not respond to amphotericin B, a common antifungal drug.
-
It is linked to high mortality when infection occurs.
🔬 What Did the Study Investigate?
Researchers in Tyrol, Austria studied where A. terreus is found in soil and why it appears more often in some areas than others.
They:
-
Collected soil samples from eastern and western Tyrol.
-
Used special techniques to detect A. terreus in the soil.
-
Analyzed factors like pH, moisture, and nutrients in the soil.
-
Compared the fungal resistance of A. terreus to different antifungal medications.
📈 What Did They Find?
1. Higher Risk in Eastern Tyrol
-
A. terreus was much more common in eastern Tyrol than in the west.
-
It was rare in other parts of Austria.
2. Linked to Soil Conditions
-
A. terreus was more likely to be found in soils with:
-
Lower pH (more acidic)
-
Less carbon and nitrogen
-
Lower soil density
-
3. Antifungal Resistance Patterns
The fungal samples were tested against common antifungal drugs:
| Drug | Resistance |
|---|---|
| Amphotericin B | 98.3% appeared treatable (wild type) – but A. terreus is known to respond poorly in real patients |
| Voriconazole | 100% treatable |
| Posaconazole | 100% resistant |
| Isavuconazole | 87.2% resistant |
💡 Why This Matters for Patients
-
If you have aspergillosis caused by A. terreus, your doctor may need to avoid certain medications, especially posaconazole and isavuconazole, due to resistance.
-
Knowing that A. terreus thrives in certain soil conditions helps researchers understand environmental risks, especially in areas like Tyrol.
-
It highlights the importance of:
-
Identifying the exact Aspergillus species
-
Testing antifungal resistance before choosing treatment
-
Monitoring soil environments in high-risk areas
-
🩺 What You Can Do
-
If you’re receiving treatment for aspergillosis, ask whether species identification and drug resistance testing have been done — especially if your symptoms are not improving.
-
If you live in or visit high-risk regions like Tyrol, take extra precautions if you are immunocompromised or have chronic lung conditions:
-
Avoid digging in soil or handling compost without a mask
-
Stay informed about local environmental risks
-
🩺 Can Blood Tests Help Diagnose and Monitor ABPA?
The published paper is entitled "Serum periostin and carcinoembryonic antigen for diagnosing and assessing response in allergic bronchopulmonary aspergillosis" and you can read it here (Pubmed).
A study looks at two inflammation markers: CEA and periostin
🌬️ What Is ABPA?
Allergic Bronchopulmonary Aspergillosis (ABPA) is a condition where the immune system overreacts to the fungus Aspergillus, leading to lung inflammation. It commonly affects people with asthma or cystic fibrosis and can be difficult to tell apart from asthma alone.
Doctors are looking for better ways to diagnose ABPA and track how well treatment is working.
🧪 What Markers Were Studied?
This study looked at two substances found in blood:
-
CEA (Carcinoembryonic Antigen) – a marker linked to inflammation and also sometimes used in cancer screening.
-
Periostin – a protein linked to type 2 inflammation, which is common in asthma and ABPA.
Researchers wanted to know:
-
Can these markers help tell the difference between asthma and ABPA?
-
Can they be used to track how well ABPA treatment is working?
👥 Who Was Studied?
-
112 people with ABPA
-
108 people with asthma only
-
All participants had their blood tested:
-
At the start
-
Two months after taking oral steroids (prednisolone)
-
📊 What Did They Find?
1. ABPA patients had higher levels of CEA and periostin
-
Median CEA levels were:
-
4.8 ng/mL in ABPA
-
2.35 ng/mL in asthma only
-
-
Median periostin levels were:
-
22.03 ng/mL in ABPA
-
16.36 ng/mL in asthma
-
2. CEA was more useful than periostin for diagnosis
-
A test's accuracy is measured using something called AUROC (Area Under the ROC Curve):
-
CEA scored 0.77 – modestly good
-
Periostin scored 0.64 – less accurate
-
3. Markers dropped after treatment – but not in everyone
-
After two months of steroid treatment:
-
CEA and periostin levels went down overall
-
However, in around 1 in 3 people, the markers actually increased
-
🩺 What Does This Mean for Patients?
-
CEA and periostin may help doctors distinguish ABPA from asthma, but they are not perfect tests.
-
CEA is slightly more reliable than periostin as a diagnostic marker.
-
These blood tests are not reliable enough to track how well treatment is working, since levels didn’t consistently go down in all patients.
-
More research is needed before these tests can be used confidently in everyday care.
✅ What You Can Do
If you're being tested for ABPA:
-
Know that diagnosis still depends on a combination of symptoms, scans, allergy tests, and blood tests, not one single marker.
-
Speak with your doctor about the full picture – including IgE levels, lung imaging, and fungal allergy testing.
8. 🌊 Aspergillosis in Dolphins and Whales: What It Tells Us About the Environment
The published paper is entitled "Aspergillus Infections in Cetaceans: A Systematic Review of Clinical, Ecological, and Conservation Perspectives" and you can read it here (Pubmed).
A growing fungal threat in marine mammals linked to climate and human impact
🐬 What’s the Issue?
Aspergillus fungi — especially Aspergillus fumigatus — are now being found in marine mammals like dolphins, porpoises, and whales. These animals, called cetaceans, are increasingly suffering from aspergillosis, a fungal disease more commonly known for affecting humans with weakened lungs or immune systems.
But this isn’t just an animal health issue — it may also be a warning sign for humans and the environment.
🔍 What Did the Review Study?
Researchers looked at 34 studies involving 106 marine mammals and found that:
-
Aspergillus infections affected:
-
The lungs and airways
-
The brain
-
The ears
-
-
Many infections were severe or fatal, especially when animals had other infections (like morbillivirus) or were exposed to pollution or climate stressors (which weaken the immune system).
⚠️ Important Findings
-
Invasive aspergillosis (where the fungus spreads through the body) was often deadly.
-
Azole-resistant Aspergillus fumigatus (the kind that resists common antifungal drugs) was found in wild porpoises — showing that environmental exposure to antifungals (e.g. from agriculture or pollution) is affecting marine life.
-
Many animals were not fully tested, meaning the true number of infections may be underestimated.
-
Stranded or sick animals often had undiagnosed fungal infections.
-
There was little discussion of how this affects conservation efforts, even though fungal disease may be harming cetacean populations.
🌍 Why Does This Matter to Us?
This research is a reminder that fungal diseases are not just a human issue. They are part of a wider pattern of:
-
Climate change
-
Environmental damage
-
Emerging infectious diseases
Cetaceans are considered “sentinel species” — meaning their health can reflect larger environmental risks that may also affect people. If they are getting sick from drug-resistant fungi, it may point to problems in our shared air, water, and ecosystems.
🩺 What’s Needed Next?
-
Better testing and species identification when marine mammals are found stranded or ill
-
Stronger antifungal resistance monitoring, including in wildlife and the environment
-
Cross-sector cooperation under a One Health approach (uniting human, animal, and environmental health)
-
Greater awareness that fungal infections like aspergillosis are growing threats in a changing climate
🐋 Key Takeaway for Patients
If you live with aspergillosis, this study may help you understand how environmental exposure and fungal resistance are global issues — affecting not just humans but animals and ecosystems too.
It reinforces why your voice as a patient matters in climate conversations, public health, and One Health research.
9. Understanding Drug Interactions with Isavuconazole (Cresemba)
The published paper is entitled "The Effect of Drug-Drug Interactions on the Pharmacokinetics of Isavuconazole: A Comprehensive Review" and you can read it here (Pubmed).
What is Isavuconazole?
Isavuconazole (brand name Cresemba) is an antifungal medicine used to treat serious fungal infections like invasive aspergillosis and mucormycosis. It works by blocking an enzyme that fungi need to grow.
Why Was This Study Done?
The study aimed to better understand how other medicines might affect the way isavuconazole works in the body — something known as drug-drug interactions (DDIs). These interactions can change how much of the drug ends up in your bloodstream, which can make it less effective or more toxic.
Key Findings for Patients
Researchers looked at 1,051 scientific articles and selected 11 high-quality studies involving 23 different drugs. Here’s what they found:
-
🟥 Some drugs reduce the effectiveness of isavuconazole:
-
Rifampicin, flucloxacillin, and phenobarbital lower the amount of isavuconazole in your body, meaning the antifungal might not work as well.
-
-
🟦 Some drugs increase the amount of isavuconazole:
-
Ketoconazole and ritonavir increase the levels, which could lead to more side effects.
-
-
🟩 Some drugs seem to have no significant effect:
-
Examples: esomeprazole (for acid reflux), digoxin, metformin, warfarin, prednisone, and methotrexate.
-
However, many of these studies were done using only a single dose, which doesn’t give a full picture. So, caution is still needed if you're taking these long-term.
-
What Does This Mean for You?
-
Drug interactions mainly affect isavuconazole through a liver enzyme called CYP3A4.
-
Some drugs speed up this enzyme (called inducers), reducing isavuconazole's effect.
-
Others slow it down (called inhibitors), raising isavuconazole levels and the risk of side effects.
-
-
If you’re taking isavuconazole long-term, especially with other medications:
-
Avoid mixing it with strong enzyme inducers or inhibitors, unless advised by a specialist.
-
Your healthcare provider may need to use therapeutic drug monitoring (TDM) — this means checking blood levels of the drug to make sure you’re getting the right dose.
-
Key Message
Always tell your doctor or pharmacist about all the medicines you take — including antibiotics, anti-epileptics, HIV medicines, herbal remedies, and over-the-counter drugs. Some can strongly affect how isavuconazole works.
This study supports careful monitoring and personalised dosing to keep treatments safe and effective.
10. 🦠 New Hope for Difficult Fungal Infections: Olorofim
The published paper is entitled "Olorofim for the treatment of invasive fungal diseases in patients with few or no therapeutic options: a single-arm, open-label, phase 2b study" and you can read it here (Pubmed).
💡 What Was This Study About?
Invasive fungal diseases (IFDs), including aspergillosis, Lomentospora, Scedosporium, and Coccidioides infections, can be life-threatening—especially when existing antifungal drugs don’t work due to resistance. This study tested a new antifungal medicine called olorofim, the first of a brand-new class called orotomides.
🧪 How Does Olorofim Work?
Olorofim attacks fungi differently from current drugs. It blocks a process that fungi need to make pyrimidines, which are essential for their survival. This kills the fungus without harming human cells.
👥 Who Was in the Study?
-
204 patients from 11 countries took part.
-
All had serious fungal infections with limited or no treatment options.
-
The most common infection was aspergillosis, including strains resistant to standard drugs.
💊 What Treatment Did They Get?
-
Everyone received oral olorofim (no placebo or comparison drug).
-
The dose was adjusted as researchers learned more during the trial.
-
Treatment lasted up to 84 days, with longer treatment allowed if needed.
📈 What Did the Study Measure?
Researchers looked at:
-
Global response (a mix of clinical signs, scans, and lab results)
-
Clinical improvement alone
-
Survival at 42 and 84 days
-
Side effects
📊 What Were the Results?
| Outcome | What Happened? |
|---|---|
| Clear improvement (strict definition) | 29% of patients improved by day 42 |
| Improvement or stable disease | 75% at day 42, 63% at day 84 |
| Clinical improvement only | 60% at day 42, 54% at day 84 |
| Survival | 88% survived to day 42; 84% to day 84 |
| Liver-related side effects | 10% had liver enzyme changes (mostly mild/manageable) |
| Stomach upset | 10%, mostly mild and short-lived |
| Treatment-related deaths | None reported |
🧠 What Does This Mean for Patients?
-
Olorofim may offer a much-needed option for people with difficult fungal infections—especially when other treatments fail.
-
Though not perfect, the drug helped many patients stay stable or improve.
-
It was generally well tolerated, with no deaths directly caused by the drug.
📌 Key Takeaway
Olorofim could become a valuable new tool in treating invasive fungal infections—especially resistant ones like azole-resistant Aspergillus. More research is still needed, but this study gives hope to patients facing limited options.
11. When NTM and Aspergillosis Occur Together: What This Study Found
The published paper is entitled "Risk Factors and Long-Term Prognosis for Coinfection of Nontuberculous Mycobacterial Pulmonary Disease and Chronic Pulmonary Aspergillosis: A Multicentre Observational Study in Japan" and you can read it here (Pubmed).
Focus: Japan, 2010–2017 | 18 hospitals | 1,304 patients
💡 What Was This Study About?
This research looked at people with nontuberculous mycobacterial pulmonary disease (NTM-PD)—a chronic lung infection that’s becoming more common worldwide.
The key question was:
How often do people with NTM-PD also develop chronic pulmonary aspergillosis (CPA), and what does this mean for their long-term health?
🔬 What Did the Researchers Do?
They studied 1,304 adults in Japan diagnosed with NTM-PD. The team looked at:
-
Who developed CPA (a long-term fungal lung infection caused by Aspergillus).
-
What risk factors increased the chance of CPA.
-
How having both conditions affected survival over time.
📊 Key Results
🦠 How Common Was CPA?
-
45 patients (3.5%) with NTM-PD also developed CPA.
-
Almost all cases were chronic progressive CPA (a serious, long-term form).
⚠️ Who Was Most at Risk?
Risk factors for developing CPA included:
-
Being male
-
Having chronic obstructive pulmonary disease (COPD)
-
Using oral steroids
-
Having cavity formations in the lungs (seen on scans)
💀 How Did CPA Affect Survival?
-
People with both NTM and CPA were 4 times more likely to die than those with NTM alone.
-
Even after adjusting for other health issues, CPA was still an independent risk factor for lower survival (hazard ratio: 1.59).
🧠 What Does This Mean for Patients?
-
NTM and CPA together are dangerous, leading to worse health outcomes than NTM alone.
-
Patients with NTM-PD who have lung cavities, are on steroids, or have COPD should be closely monitored for signs of CPA.
-
Early diagnosis and treatment of CPA may help improve quality of life and survival.
📌 Key Takeaway
Chronic pulmonary aspergillosis is a serious complication of NTM lung disease. Doctors should be alert to the risk, especially in high-risk individuals, so they can start treatment early and possibly improve outcomes.
12. Bronchial Artery Embolisation: What Patients Should Know
The published paper is entitled "Long-term outcomes following embolisation of bronchial and non-bronchial systemic arteries for the management of haemoptysis - a 20-year experience" and you can read it here (Pubmed).
Study: 20 Years of Experience in a London Teaching Hospital (2002–2022)
💡 What Was This Study About?
This study looked at how effective and safe bronchial artery embolisation (BAE) is for treating people who cough up large amounts of blood (moderate to massive haemoptysis), a medical emergency in many cases.
The team also wanted to understand:
-
How often bleeding comes back (recurrence)
-
What health conditions make recurrence more likely
-
How often serious complications (like stroke) happen
🩺 What Is BAE?
BAE is a non-surgical procedure that blocks the bleeding blood vessels in the lungs. It’s often used when patients are too ill for surgery or as a first-line treatment when bleeding is life-threatening.
📊 What Did the Study Find?
✔️ Effectiveness
-
Technical success (the procedure worked as intended): 88%
-
Clinical success (bleeding stopped): 85%
🔁 Recurrence
-
Bleeding came back in 46% of cases.
-
20 patients needed the procedure again.
⚠️ Higher risk of recurrence in patients with:
-
Aspergilloma (a fungal ball, usually from Aspergillus)
-
Cystic fibrosis
-
Non-tuberculous pneumonia
These patients are more likely to have long-term lung damage and cavitations (holes or pockets in the lungs), which makes bleeding more likely to return.
🧠 Stroke Risk
-
Stroke occurred in 6.4% of patients – higher than usually reported.
-
Most strokes were in people with lung cavities from infection (e.g., aspergilloma or pneumonia).
📌 What Does This Mean for Patients?
-
BAE is often life-saving for severe lung bleeding and avoids major surgery.
-
However, the bleeding may return, especially if you have certain lung diseases.
-
There is a small but serious risk of stroke, especially in patients with lung cavities caused by infection.
-
A detailed consent process is essential before BAE, including a discussion of stroke risk and recurrence.
🧠 Key Takeaway
Bronchial artery embolisation is effective, but not without risks.
If you have aspergilloma, cystic fibrosis, or chronic lung infection, you may:
-
Need careful monitoring after the procedure
-
Be at increased risk for bleeding to come back
-
Face a higher risk of complications like stroke
13. 🦠 Aspergillus Lung Infections: What This Study Found in a Major French Hospital
The published paper is entitled "Pulmonary Aspergillosis: Epidemiology and unresolved diagnostic challenges - insights from a two-year retrospective cohort study in Marseille" and you can read it here (Pubmed).
Study period: January 2022 – December 2023
💡 What Was the Study About?
The Aspergillus fungus is common in the environment and can cause different lung diseases, depending on your immune system:
-
Invasive pulmonary aspergillosis (IPA) – usually in people with weakened immune systems
-
Chronic pulmonary aspergillosis (CPA) – long-term infection in people with existing lung conditions
-
Allergic bronchopulmonary aspergillosis (ABPA) – an allergic response in people with asthma or cystic fibrosis
This study aimed to understand how common these diseases are, how they are diagnosed, and how well they are managed in a large hospital in Marseille, France.
🔬 What Did the Researchers Do?
They reviewed data from thousands of patients who had tests for Aspergillus infection:
-
Galactomannan (GM) antigen test – mainly for detecting IPA
-
Aspergillus-specific IgG – helps diagnose CPA
-
Aspergillus-specific IgE – used for ABPA diagnosis
They also looked at patients’ medical records, imaging, and outcomes, using standard criteria to make diagnoses.
📊 Key Findings
| Condition | Cases Diagnosed | % of Those Tested | 3-Month Mortality |
|---|---|---|---|
| IPA | 46 out of 2,412 | 1.9% | 46.7% |
| CPA | 16 out of 2,889 | 0.6% | 13.3% |
| ABPA | 46 out of 1,779 | 2.6% | 0% (but 13% worsened) |
⚠️ Additional Observations
-
Newer immune-suppressing drugs like tocilizumab and oblinutuzumab may be emerging risk factors for IPA.
-
Only 10 out of 46 people with ABPA were actually treated by a doctor, suggesting many cases are missed or undertreated.
-
This shows a gap between guidelines and real-world practice, especially for ABPA.
🧠 What Does This Mean for Patients?
-
IPA and CPA can be deadly, especially without early diagnosis and proper treatment.
-
ABPA is often under-recognised, even though it is treatable and doesn’t usually cause death. However, if left untreated, symptoms can worsen.
-
Better testing and awareness are needed, especially for people with asthma, cystic fibrosis, or weakened immune systems.
-
If you have symptoms like long-term cough, breathlessness, or recurring infections — especially with known lung conditions — it’s worth discussing Aspergillus testing with your doctor.
📌 Key Takeaway
Aspergillus lung diseases are real and serious — but often missed or under-treated.
Improved testing, awareness, and up-to-date treatment decisions are urgently needed to save lives and improve care, especially for ABPA patients who are often overlooked.
14. 🧪 Study Summary: How Does CPA Affect People with HIV?
The published paper is entitled "Chronic Pulmonary Aspergillosis in People Living with HIV: An Uncommon and Under-Recognized Association" and you can read it here (Pubmed).
🦠 What Is CPA?
Chronic pulmonary aspergillosis (CPA) is a long-term fungal lung infection, usually affecting people who already have damaged lungs — such as from TB (tuberculosis), asthma, bronchiectasis, or COPD. It's caused by a common fungus called Aspergillus, which we all breathe in every day, but which can become harmful in people with weakened lungs or immune systems.
📚 What Did This Study Look At?
Researchers in São Paulo, Brazil, looked back at the records of 96 people diagnosed with CPA between 2010 and 2024 to understand:
-
How CPA affects people living with HIV (PLHIV)
-
How they respond to treatment
-
Whether they have different risks or outcomes than other patients
👥 Who Was in the Study?
-
8 patients (8%) had HIV
-
88 patients (92%) did not have HIV
-
All had a confirmed diagnosis of CPA based on recognised international criteria
🔍 What Did They Find?
📊 Differences in HIV-Positive vs HIV-Negative CPA Patients:
| Factor | PLHIV (with HIV) | HIV-Negative |
|---|---|---|
| Median age | 44 years | 52 years |
| Had active TB | 38% | 4.5% |
| Used itraconazole (antifungal) | 57% | 79% |
| 1-year mortality | 13% | 4% |
| Clinical failure rate | 50% | Not specified |
💡 What Does “Clinical Failure” Mean?
It means the patient did not improve or worsened despite treatment, such as:
-
Long-term antifungal medication (like itraconazole)
-
Surgery (such as lung resection)
Half of the people living with HIV in this study experienced clinical failure — a worryingly high rate.
🧠 Key Messages for Patients:
-
CPA can occur in people with HIV, especially if they've had TB.
-
Diagnosis may be delayed or missed, because HIV and TB can complicate the picture.
-
Treatment may not always work well — even with antifungal medication and surgery, some people don’t improve.
-
More research is needed to find better ways to treat CPA in people with weakened immune systems, like those with HIV.
❤️ What Can Patients Take Away?
If you live with HIV and have had TB or other lung infections, and you're experiencing symptoms like:
-
Persistent cough
-
Fatigue
-
Weight loss
-
Coughing up blood
-
Chest pain
…then CPA could be part of the picture, and it’s worth asking your specialist whether this has been considered.
15. 🧬 How the Immune System Responds in Chronic Pulmonary Aspergillosis (CPA)
The published paper is entitled "Dendritic cell dysfunction, including impaired IL-12 production, is associated with chronic pulmonary aspergillosis" and you can read it here (Pubmed).
New research uncovers why some immune responses may fail to control this fungal infection
🦠 What Is CPA?
Chronic pulmonary aspergillosis (CPA) is a long-term fungal infection of the lungs caused by the Aspergillus fungus. It mostly affects people with already damaged lungs, like those with bronchiectasis, asthma, TB scars, or COPD.
Doctors know that the immune system is involved in whether CPA develops or not—but this study aimed to understand exactly how the immune system behaves differently in CPA patients.
🧪 What Did the Researchers Do?
-
They looked at 25 patients with CPA and 25 people with bronchiectasis but no CPA (as a comparison group).
-
They collected blood samples and studied how immune cells behaved both:
-
At rest
-
After being "stimulated" in the lab using a substance that mimics fungal infection (Zymosan)
-
This allowed them to see how well different immune cells responded to a fungal challenge.
🔬 Key Findings
1. CPA Patients Had More Neutrophils
-
These are inflammatory white blood cells often found in infection.
-
High numbers can mean ongoing inflammation but also may reflect a less specific immune response.
2. Weaker Dendritic Cell (DC) Response
-
Dendritic cells act like "messengers" in the immune system.
-
In CPA patients, key DC types were reduced in number and showed weaker activity.
-
They produced less IL-12 and TNFα (important for fighting fungi and viruses)
-
They showed less CD86, a protein needed to "wake up" other immune cells
-
This suggests CPA patients' immune systems struggle to mount a strong, coordinated response.
3. Possible Link to Low Interferon Gamma (IFNγ)
-
These weak responses might explain low IFNγ levels, previously linked to poor fungal control in CPA.
-
IFNγ is vital for helping the body control fungal and bacterial infections.
4. TB History May Affect Immunity
-
Patients who had TB in the past had more activated immune cells — possibly due to “innate immune memory” (the immune system “remembers” past infections and responds differently).
🧠 Why Is This Important for Patients?
-
It helps explain why CPA develops in some people and not others with similar lung damage.
-
It shows that CPA is not just about having fungus in the lungs — it's about how the immune system fails to respond effectively.
-
It supports other studies suggesting that some CPA patients could benefit from immune-boosting treatments, like interferon gamma therapy (currently under investigation).
-
It also suggests a history of TB might leave lasting changes in how the immune system reacts to fungi.
🧭 What Could This Mean in the Future?
-
Better blood tests to identify people at risk of developing CPA
-
New treatments that target the immune system, not just antifungals
-
Improved understanding of why some patients don’t respond to antifungals alone
❤️ Summary for Patients
People with CPA may have immune cells that don’t work properly, especially cells that are supposed to trigger the body’s antifungal response. This means they can’t control Aspergillus as well as others, even if their lungs are damaged in similar ways. Past infections like TB might leave immune "memories" that change how the body reacts to fungi in the future.
16. 🖥️ What Can a CT Scan Tell Us About CPA?
Understanding lung scans in chronic pulmonary aspergillosis (CPA)
🧠 What Was the Study About?
This study looked at CT (computed tomography) scans from over 100 people with chronic pulmonary aspergillosis (CPA), to see how the condition appears in the lungs—and whether scan results could help doctors tell the different subtypes of CPA apart.
📊 Who Was In the Study?
-
103 people with CPA
-
Average age: 47
-
Majority were men (69 out of 103)
-
Most had previous tuberculosis-related lung damage (97%)
🦠 What Are the Types of CPA?
| CPA Subtype | Description | Percentage in study |
|---|---|---|
| Chronic Cavitary Pulmonary Aspergillosis (CCPA) | Multiple cavities in the lungs without major fibrosis | 77.7% |
| Chronic Fibrosing Pulmonary Aspergillosis (CFPA) | Advanced scarring and shrinkage of the lungs | 15.5% |
| Simple Aspergilloma | A single fungal ball inside one cavity | 6.8% |
🔍 What Did the CT Scans Show?
| Feature | Key Findings |
|---|---|
| Cavities | Found in 100% of patients; often in the left upper lobe |
| Cavity wall thickness | Median 6mm overall; thicker in CFPA |
| Multiple cavities | Seen in 87.5% of CFPA vs 41.5% of CCPA cases |
| Intracavitary contents | (like fungal balls or debris) in 89.3% of patients |
| Pericavitary fibrosis (scarring) | Seen in 71% overall; 100% in CFPA |
| Pleural thickening | Median 8mm, worse in more advanced CPA |
| Mediastinal shift | Lung shrinking in CFPA sometimes pulls chest structures sideways |
| Posterior lymph nodes | Found in 66% — a new potential sign of CPA on scans |
🤔 What Does This Mean for Patients?
-
CT scans are essential in diagnosing and understanding CPA.
-
Different subtypes of CPA show different patterns on scans—for example:
-
More cavities and fibrosis in CFPA
-
Single, isolated cavities in aspergilloma
-
-
Recognising these differences helps doctors:
-
Choose the right treatment (antifungals, surgery, monitoring)
-
Track disease progression
-
Plan for lung preservation
-
🗣️ Doctor–Patient Tip:
"When looking at my CT results, can you help me understand what type of CPA I have? Does the scan show fibrosis, single or multiple cavities, or signs of shrinkage?"
💡 Final Thought
This study shows that a careful review of CT scans — not just a quick look — can offer important clues about the severity, type, and likely progression of CPA. As imaging improves, patients and clinicians can work together to spot changes early and make informed decisions about treatment.

🧬 Are Vaccines for Aspergillosis on the Horizon?
If you live with aspergillosis—whether it's ABPA (Allergic Bronchopulmonary Aspergillosis), CPA (Chronic Pulmonary Aspergillosis), or invasive aspergillosis—you’ve probably wondered if a vaccine might one day help prevent or control this condition. As of 2025, there is no licensed vaccine for any form of aspergillosis, but scientists are actively working on it.
This article explains where things stand, what’s being developed, and what it could mean for people like you.
🦠 What is Aspergillosis?
Aspergillosis is a group of illnesses caused by the fungus Aspergillus fumigatus. It’s very common in the environment, especially in soil, dust, and decaying vegetation. Most people breathe in the spores without getting sick, but if you have:
-
Damaged lungs (due to asthma, COPD, or TB)
-
A weakened immune system
-
An allergic reaction to fungal spores
…you may develop a form of aspergillosis, such as:
-
ABPA – a severe allergic lung condition
-
CPA – long-term fungal infection in damaged lungs
-
Invasive aspergillosis – a fast-moving, life-threatening infection in immunocompromised people
💉 Why Develop a Vaccine?
A vaccine could:
-
Prevent serious illness in high-risk people (like cancer or transplant patients)
-
Reduce allergic sensitisation in ABPA
-
Lower the need for long-term antifungal drugs, which can have side effects and lose effectiveness
-
Protect against lung damage caused by repeated infections
But making a vaccine isn’t easy—especially for a disease that behaves differently depending on a person’s immune system.
🧪 Vaccines in Development (2025)
While none are yet available for patients, several experimental vaccines are being tested in laboratories and early-stage trials. Here are the most promising ones:
1. NDV-3A Vaccine
-
Originally developed for a yeast infection (Candida albicans)
-
Found to trigger cross-protection against Aspergillus fumigatus
-
Uses a protein called Als3p, shared between fungi
-
Completed early safety trials for Candida
-
Being explored for people with weak immune systems, like transplant recipients
2. AF.KEX1 DNA Vaccine
-
Uses a fungal protein called Kexin 1
-
Delivered as a DNA vaccine to help the body produce protective immune cells
-
Shown to work well in animal models
-
Designed to help high-risk patients, such as those having chemotherapy
3. Asp f3 Protein Vaccine
-
Focuses on a specific Aspergillus protein (Asp f3)
-
Stimulates T-helper cells (Th1 and Th17), important for fighting fungal infections
-
Still in preclinical stages, but results in mice are promising
4. Nasal Spray Vaccine with Nanoparticles
-
Uses chitosan (a natural substance) to deliver the vaccine via the nose
-
Aims to stimulate mucosal immunity (lining of the lungs and airways)
-
Could be useful for people with ABPA or cystic fibrosis, who often have fungal colonisation in the lungs
5. Exploratory mRNA Vaccines
-
Inspired by COVID-19 vaccine technology
-
Still experimental, but may offer faster, more targeted vaccine design
-
No clinical trials yet, but research is underway
🚧 Why Don’t We Have a Vaccine Yet?
Developing a vaccine for aspergillosis is challenging:
-
The immune response needed varies between allergic, chronic, and invasive forms
-
Many people most at risk (e.g. after organ transplant) are too immunocompromised to respond well to vaccines
-
Aspergillus has many different proteins—no single target works for everyone
-
Research funding is often limited, because aspergillosis is considered rare
👥 Who Might Benefit Most?
A future vaccine could be life-changing for:
-
People with weakened immune systems (e.g. after stem cell or organ transplant)
-
People with long-term lung disease, including ABPA and CPA
-
Children and adults with cystic fibrosis
-
People undergoing chemotherapy or immune-suppressing treatment
🗣️ What Can Patients Do?
You can help push this research forward:
-
Join a registry or research study if asked by your hospital
-
Share your story with groups like the National Aspergillosis Centre (NAC) or Rare Disease UK
-
Support advocacy efforts calling for better funding of fungal research
-
Stay up to date with trial opportunities on trusted sites like aspergillosis.org
📌 Key Takeaways
| Question | Answer |
|---|---|
| Is there a vaccine for ABPA or CPA? | Not yet — but several are in development. |
| Who might benefit from a vaccine? | People with asthma, CF, CPA, ABPA, or weakened immunity |
| When will it be available? | Likely several more years away — still early in trials |
| What’s the biggest challenge? | Complex immunity, rare disease status, limited funding |
🧭 Looking Ahead
Although no vaccine is available yet, the science is moving forward — thanks to global research teams who see the impact aspergillosis has on patients’ lives. Even small steps now could lead to major breakthroughs in future care.
Your voice matters. Stay connected, stay informed — and keep asking for more focus on this important condition.
How can we, as patients, support or raise our voices to bring more focus to ABPA in the medical and research world?
You're absolutely right that ABPA (Allergic Bronchopulmonary Aspergillosis) often sits in the shadow of more widely recognised diseases like asthma, cystic fibrosis, and even chronic pulmonary aspergillosis (CPA), despite the daily impact it has on breathing, energy, and quality of life for those affected. Here's a comprehensive response to your two key questions:
👉 Is more active research or clinical development happening specifically for ABPA therapies?
✅ Some research is happening — but it's limited and fragmented.
-
ABPA is considered a rare disease (likely fewer than 10,000 diagnosed in the UK), so it doesn’t attract the same commercial research attention as asthma, cystic fibrosis (CF) or chronic obstructive pulmonary disease (COPD)..
-
ABPA overlaps with asthma, cystic fibrosis, and bronchiectasis, which means treatments often come from those areas — but are not tailored to ABPA patients.
💊 Existing therapies are adapted, not designed for ABPA:
-
Steroids (oral or inhaled) remain first-line, but long-term use has harmful side effects.
-
Azole antifungals (like itraconazole or voriconazole) are used to reduce fungal burden — but responses vary, side effects are common, and resistance is rising.
-
Biologics (like omalizumab, mepolizumab, dupilumab, and now tezepelumab) are showing promise in small studies and real-world experience — but none are licensed specifically for ABPA, which means access is inconsistent and often requires individual funding requests (IFRs).
🔬 Ongoing research and development (as of 2025):
-
Japan and India are leading some ABPA-specific studies, especially around imaging, IgE trends, and steroid-sparing strategies.
-
Small studies and case series are evaluating biologic therapies in ABPA, particularly in:
-
Asthma + ABPA overlap
-
CF + ABPA overlap
-
Bronchiectasis + ABPA cases with poor control
-
-
No current large-scale Phase 3 trials for ABPA-specific therapies are active in the UK or Europe, though there is growing academic interest at centres like Manchester (NAC) and Royal Brompton and specialist centres across Europe.
👉 How can we, as patients, raise our voices to bring more focus to ABPA?
🗣️ 1. Share your story
-
Personal experiences — like the one you just shared — are powerful advocacy tools. NAC and Aspergillosis Trust are regularly asked to provide volunteers to talk about their experiences for national media stories - when they happen there is usually little time to respond so leaving your contact details with Aspergillosis Trust or NAC can be a way to help raise awareness.
-
Blogs, social media, patient interviews, or videos can humanize the condition for researchers, clinicians, and policymakers.
-
You could contribute to aspergillosis.org, BLF, or Rare Disease UK platforms.
💬 2. Engage with research centres
-
The National Aspergillosis Centre (NAC) is uniquely placed to drive research.
-
Ask to be part of patient advisory panels, surveys, or focus groups — your lived experience helps shape research priorities. There is currently a Europe-wide group run by the European Lung Foundation (Aspergillosos PAG) that is designed to do exactly this, and here at NAC we periodically ask for volunteers to help run clinical trials in the UK, usually via our Facebook or Telegram groups.. The Aspergillosis Trust are also occasionally asked to suggest volunteers for trials, so it is well worth engaging with them too. There is no obligation, just join to see what is going on! Every extra person in advocacy groups gives the group more awareness power.
-
Inquire whether NAC is seeking trial participants, or if they plan to study ABPA-specific uses of biologics.
✍️ 3. Support and pressure through policy
-
Add your voice to calls for biologic licensing for ABPA.
-
Back campaigns like Accelerating Access to Rare Disease Therapies (via Genetic Alliance or Rare Disease UK).
-
Contact your local MP or ICB (Integrated Care Board) to raise access issues — such as Individual Funding Request (IFR) delays or biologic refusals.
🤝 4. Connect with others
-
ABPA-specific support groups (e.g. through NAC, Facebook groups, or Zoom meetups) allow patients to:
-
Share coping strategies
-
Create collective pressure
-
Support research studies via recruitment or funding
-
📈 5. Help build data
-
ABPA is under-diagnosed and under-coded in NHS data — meaning we don’t know how many people truly have it.
-
Participating in registries, audits, or quality-of-life research helps build a case for investment and clinical guidelines.
✨ Final Thoughts
You are right to point out that the scale of suffering from ABPA is real — even if it doesn't generate headlines. That makes patient voices even more essential. The good news is: the more we talk about ABPA, the more momentum we can build. Already, biologics are gaining attention — but formal ABPA trials, compassionate-use programs, and NHS funding clarity are still needed.
Let me know if you'd like help writing a patient statement, connecting with a researcher, or forming a focus group to bring these issues forward. You could help shape the next chapter of ABPA care.
You're doing more than you realise by speaking out. 👏
🌿 Practical Steps for Managing Steroid-Related Facial Swelling
🧊 1. Cold Compresses
-
Applying a cool, damp cloth or cold gel mask to your face and neck for 10–15 minutes may help reduce inflammation and redness, especially in the evening.
-
Avoid ice directly on the skin.
🛌 2. Elevation and Sleep Position
-
Try sleeping with your head elevated on an extra pillow. This helps reduce overnight fluid pooling in the face.
-
During the day, keep your head upright when sitting or resting.
💧 3. Fluid Management
-
Paradoxically, drinking plenty of water helps your body excrete excess salt and reduce fluid retention.
-
Consider reducing your sodium intake, as salt encourages water retention and worsens facial puffiness.
🍽️ 4. Diet Adjustments
-
Avoid high-carb and sugary foods, which can worsen fluid retention and blood sugar instability (already affected by steroids).
-
Add potassium-rich foods (e.g. bananas, spinach, sweet potatoes), which help balance fluid levels.
🚶 5. Gentle Movement
-
Short walks or mild activity during the day help circulation and prevent dependent edema (swelling that increases as the day goes on).
🧴 6. Skin Soothing and Anti-Inflammatory Topicals
-
Use fragrance-free soothing moisturisers containing niacinamide or aloe vera.
-
Redness may also respond to mild over-the-counter hydrocortisone cream for short use — though caution is advised since you're already on systemic steroids.
💊 7. Medication Review
-
Diuretics (water tablets) are rarely used for steroid-induced swelling, but in some cases, a clinician may consider it if fluid retention is severe.
-
Tapering your corticosteroids (if appropriate and under supervision) can gradually improve symptoms — discuss this with your prescriber.
🩺 8. Consult a Specialist
-
If the swelling is asymmetric, very painful, or associated with new symptoms (e.g., visual changes, difficulty swallowing, skin tightness), you should be checked promptly for other causes.
-
A referral to a dermatologist or endocrinologist may help if cosmetic or systemic effects are severe or long-term.
⚠️ When to Seek Urgent Medical Advice
Call your GP or attend an urgent care clinic if you have:
-
Sudden, painful swelling
-
Shortness of breath
-
Swelling spreading rapidly
-
New rash, fever, or visual disturbance