
🫁 The FeNO Test: What It Means for People with Aspergillosis
If you have aspergillosis, particularly ABPA (Allergic Bronchopulmonary Aspergillosis) or overlapping asthma, your doctor might suggest a test called FeNO. But what is it—and is it useful for people like you?
This guide explains the FeNO test in simple terms, how it works in patients with aspergillosis, and what to expect from the results.
🔍 What Is the FeNO Test?
FeNO stands for Fractional Exhaled Nitric Oxide. It’s a quick and painless breathing test that measures the level of nitric oxide gas in your breath.
Nitric oxide is naturally produced in your lungs. When your airways are inflamed—especially with eosinophilic (type 2) inflammation—levels go up.
This kind of inflammation is common in:
-
Asthma
-
Allergic Bronchopulmonary Aspergillosis (ABPA)
-
Some cases of chronic aspergillosis with allergic features
🎯 Why Might Aspergillosis Patients Be Offered a FeNO Test?
Your team might use FeNO to:
-
Support a diagnosis of ABPA or allergic asthma
-
Monitor inflammation levels over time
-
Check if inhaled steroids are working
-
Help plan changes to your treatment
FeNO can help show how much inflammation is active in your lungs, even if your symptoms haven’t changed much.
📈 Is the FeNO Test Accurate?
FeNO is a proven and recommended tool in asthma and allergic lung disease, including ABPA. But it works best when used alongside other information—such as:
-
Blood tests (like total and specific IgE)
-
CT scans
-
Lung function tests
-
Sputum cultures and fungal markers
So FeNO doesn’t give a “yes” or “no” answer by itself. It’s part of the bigger picture.
⚠️ What Can Affect the Results?
Certain things can raise or lower your FeNO level:
-
Smoking (lowers it)
-
Recent steroid use (lowers it)
-
Recent infections
-
Foods rich in nitrates (like beetroot, spinach)
-
ABPA flares (may raise it)
This is why your clinician will always interpret your FeNO result in context.
🩺 Should You Trust It?
Yes — when interpreted by an experienced team, FeNO is a safe and useful tool. It helps in understanding how allergic inflammation behaves in your lungs, especially if you're living with ABPA or asthma alongside aspergillosis.
✅ Summary for Aspergillosis Patients
-
FeNO is helpful in allergic forms of aspergillosis, like ABPA
-
It measures airway inflammation, especially type 2 (eosinophilic) inflammation
-
It helps guide treatment with inhaled steroids or biologics
-
It’s not a stand-alone test—it’s used together with other clinical information
-
If you’re unsure what your FeNO result means, just ask your care team
If you’re being treated at the National Aspergillosis Centre, or referred for specialist care, FeNO testing may be used to help plan or fine-tune your treatment.
🌿 Living with Chronic Pulmonary Aspergillosis (CPA):
Hope, Setbacks, and What “Cure” Really Means
Being diagnosed with chronic pulmonary aspergillosis (CPA) is often overwhelming. You may be on treatment with antifungals like itraconazole (Sporanox) and have already gone through ups and downs — early improvement, then a period of stagnation, and now you're facing a new CT scan with anxiety.
You’re not alone — and this guide brings together the key questions patients often ask, along with helpful real-life insights.
✅ “I Felt Better at First — Then It Stalled. Why?”
This is very common in CPA. In the first few months:
-
Symptoms like cough, breathlessness, and fatigue may improve.
-
CT scans may show fungal balls shrinking or disappearing.
But then: -
Symptoms return or stay the same.
-
Scans show little change.
-
Anxiety grows.
This doesn’t mean treatment has failed.
It may just mean you've reached a slower phase of healing. Here's why:
| Reason | What’s Happening |
|---|---|
| Antifungal success at first | Fungal load drops, but scarring and inflammation remain. |
| Itraconazole is working | But drug levels may be too low — monitoring is essential. |
| Other lung conditions coexist | Like bronchiectasis or NTM, which antifungals don’t treat. |
| Ongoing exposure to mould | Especially from damp buildings, compost, or dust. |
| Immune response adapts | Symptoms may persist even if fungus is under control. |
🔁 “Can Things Improve Again?”
Yes — many people improve again after a plateau or setback.
What helps:
-
✅ Check your itraconazole blood level — low levels = poor response.
-
✅ Consider a switch to another antifungal, like voriconazole or posaconazole.
-
✅ Ask your team about co-infections, inhaled therapies, or lung physiotherapy.
-
✅ Monitor your vitamin D, weight, and steroid use (to rule out other causes of symptoms).
-
✅ Keep going — many people improve again with time, adjustments, and support.
🗣️ “I had a dip after three months. We checked my drug levels — they were low. After a small dose change, I felt better again.” — Patient story
💬 “Can CPA Be Cured?”
🩺 What Do We Mean by “Cure”?
In medicine, a cure usually means:
-
The disease is gone,
-
Treatment is no longer needed,
-
There’s no sign of the illness coming back.
But in CPA, a full cure is rare — because the conditions that allowed it to take hold usually remain.
⚠️ Why CPA Is Rarely “Cured” in the Traditional Sense
-
CPA often happens in lungs already damaged by:
-
Tuberculosis (TB)
-
COPD or emphysema
-
Bronchiectasis
-
Allergic bronchopulmonary aspergillosis (ABPA)
These conditions are chronic and don’t disappear, even if the fungus is controlled.
-
-
Scars, cavities, and weakened lung tissue remain, and symptoms can return if antifungal treatment is stopped too soon or if reinfection occurs.
✅ So What’s a More Accurate Way to Think About It?
Instead of talking about a cure, specialists use words like:
| Term | What It Means |
|---|---|
| Clinical improvement | You feel better, symptoms reduce, scans look more stable. |
| Stability | The disease is under control — not progressing. |
| Remission | The infection is quiet or inactive — with or without treatment. |
| Disease control | Long-term treatment is helping manage the condition safely. |
📌 Think of CPA like asthma or diabetes — not "gone," but often well controlled.
🟢 Sometimes — CPA can be cured
In a small number of people:
-
The fungus is cleared completely,
-
Symptoms resolve,
-
Antifungals are stopped and not needed again.
This is more likely when:
-
CPA is caught early,
-
The disease is limited to one area,
-
The person has otherwise healthy lungs.
🟡 For Most — CPA is treatable but long-term
You may not fully “get rid of it” — but you can:
-
Live well with it,
-
Keep symptoms under control,
-
Avoid major complications.
🔴 If untreated, CPA can progress
-
Damage spreads,
-
Bleeding may worsen,
-
General health may decline.
That’s why staying on treatment and having regular check-ups is so important.
🔪 What About Surgery?
Surgery can help in some cases — but it depends on your specific situation.
🟢 Surgery may help if:
-
You have a single aspergilloma (fungal ball).
-
You're experiencing repeated bleeding (haemoptysis).
-
The lesion is growing or pressing on nearby structures.
-
Antifungals haven’t worked, or aren’t tolerated.
In these cases, removing part of the lung may stop bleeding, reduce symptoms, and improve quality of life.
🔴 Surgery may not be suitable if:
-
Disease affects both lungs or multiple areas.
-
Your lung function is too low.
-
The lesion is too close to vital structures.
-
You have underlying conditions like COPD, bronchiectasis, or ABPA that wouldn’t improve after surgery.
🩺 If surgery isn’t an option:
You may still benefit from:
-
Bronchial artery embolisation (BAE) — a non-surgical way to stop bleeding.
-
Ongoing antifungal therapy.
-
Symptom management through breathing support and physiotherapy.
💬 What Other Patients Say
| Patient Story | Outcome |
|---|---|
| “My fungal ball vanished after 6 months. I’m still on meds but doing well.” | Stable with long-term itraconazole |
| “I plateaued, then improved again after switching drugs.” | Switched to posaconazole |
| “I had surgery after coughing up blood for months. It made a huge difference.” | Surgery successful |
| “I live with scarring, but I’m off meds now and stable.” | Clinical remission |
🧾 What You Can Do
-
✅ Ask your doctor to check your itraconazole level if not already done.
-
✅ Record weekly symptoms — cough, fatigue, breathlessness.
-
✅ Ask about sputum tests for fungi or bacteria.
-
✅ Discuss surgery or embolisation if you’re coughing up blood.
-
✅ Stay hopeful — CPA is manageable, and some people do recover.
❤️ Final Thoughts
CPA is rarely curable in the strictest sense, but that doesn’t mean it’s hopeless.
Many people live full lives with the disease under control. Even if CT scans show lasting changes, what really matters is:
How you feel. How well you breathe. How stable your condition stays.
With antifungal therapy, expert care, and the right support, you are not alone — and you can feel better again.

Article 4: Why This New Information on Biofilms Can Be Reassuring — Not Frightening
💬 A Message to Patients: Why This New Information Can Be Reassuring — Not Frightening
We understand that learning about things like biofilms, the lung microbiome, or how different bugs work together might feel a little overwhelming or even alarming. These topics are complex and unfamiliar to many.
But we want you to know: this science is already improving care for people with aspergillosis — and you don’t need to understand every detail for it to help you.
✅ Examples of How Biofilm Awareness Is Already Helping Patients
🧪 1. Combined Treatment for Coinfection
People who have both Aspergillus and Pseudomonas infections are now more likely to be:
-
Tested for both microbes
-
Given combination therapy (e.g. antifungals + inhaled antibiotics)
This reduces the risk of persistent symptoms and lowers the chance of hospital admission.
🌬 2. Inhaled Therapies That Reach Biofilms
Doctors are now using or trialling inhaled medications that can:
-
Reach fungal and bacterial biofilms more directly
-
Work even when oral drugs can’t penetrate
For example, inhaled colistin or tobramycin is used in bronchiectasis; inhaled antifungals (like opelconazole) are in trials for aspergillosis.
💡 3. Chest Physiotherapy and Mucus Clearance
Biofilm research has shown that many infections hide in thick mucus. So, clearing mucus isn't just for comfort — it’s a critical part of treatment.
-
More patients now receive airway clearance devices
-
Some are referred for specialist physiotherapy to support this
🧼 4. Better Infection Control in Hospital
Because we understand that biofilms form on equipment and even in hospital air systems, specialist centres like NAC use:
-
HEPA-filtered rooms
-
Strict protocols to prevent airborne contamination
This lowers the risk of acquiring new fungal infections during hospital stays.
📊 5. More Personalised Care
Some patients now receive tailored treatment plans based on:
-
Sputum cultures that show which organisms are present
-
Whether biofilm-forming species are involved
-
Coexisting inflammation, allergies, or colonisation patterns
This is a big shift from one-size-fits-all prescriptions.
💬 Final Reassurance
These discoveries don’t mean there’s something worse going on. They mean that:
Doctors now understand more
Treatments are becoming more precise
We can often treat fewer times, more effectively
You're not alone — and you're not expected to keep up with every detail. This information helps your care team make better choices for you, reduce flare-ups, and improve quality of life. And that’s what really matters.
📝 Article 3: When Microbes Work Together – Aspergillus, Pseudomonas, and Lung Inflammation
🤝 Not all microbes are rivals — some collaborate
Recent research shows that Aspergillus fumigatus and Pseudomonas aeruginosa can cooperate, particularly in people with weakened lungs or structural damage (e.g. from bronchiectasis, CF, or CPA).
Examples of how they interact:
-
Pseudomonas produces toxins (phenazines) that sometimes stimulate Aspergillus growth in low doses
-
Aspergillus produces substances like gliotoxin that weaken immune responses and protect both microbes
-
Both can form mixed biofilms, making them more drug-resistant and more inflammatory
⚠️ Clinical implications:
Coinfection with Aspergillus and Pseudomonas is associated with:
-
Worse lung function in CF, bronchiectasis, CPA
-
More frequent exacerbations and hospital admissions
-
Longer recovery times and lower quality of life
🧠 Why is this important for treatment?
Doctors are now:
-
Testing for multiple microbes during exacerbations
-
Using combination therapy — antifungals and antibiotics together
-
Supporting the immune system with:
-
Airway clearance
-
Nutrition
-
Steroid balancing (not too much, not too little)
-
🧬 New tools on the horizon:
-
Drugs that block microbial signalling (quorum sensing)
-
Microbiome profiling to predict flare-ups
-
Biofilm-dissolving agents in development
-
Inhaled antifungals under trial (e.g. opelconazole)
🌟 Final Summary: A Shift in Perspective
| Old Approach | New, Holistic Approach |
|---|---|
| Target a single infection | Understand the whole lung ecosystem |
| Treat only during active infection | Focus on prevention, balance, resilience |
| One-size-fits-all antibiotic use | Tailored therapy, minimise microbiome damage |
| Ignore biofilms | Disrupt biofilms and support mucus clearance |
| Fungal and bacterial issues separate | Recognise synergy and co-infection |

📝 Article 2: The Lung Microbiome – More Than Just Aspergillus
🌱 What is the lung microbiome?
The lung microbiome is the collection of bacteria, fungi, and viruses that naturally live in your respiratory system. For a long time, lungs were thought to be sterile — we now know that they host complex microbial communities, even in healthy people.
In people with chronic lung conditions like CPA, ABPA, asthma, bronchiectasis, and cystic fibrosis, the lung microbiome can become unbalanced. Certain harmful microbes may overgrow, while beneficial ones disappear.
🤝 Why is this important?
The balance of microbes in your lungs affects:
-
How your immune system responds
-
Whether inflammation is triggered or controlled
-
How easily infections take hold
In aspergillosis patients:
-
Disruption of the microbiome may encourage fungal growth
-
Frequent antibiotics (for chest infections) can kill good bacteria, giving fungi and drug-resistant bacteria an advantage
-
Some microbes may protect against Aspergillus or help modulate inflammation
This is particularly important during flare-ups and exacerbations.
🧪 What are researchers doing?
Lung microbiome research is growing rapidly. Scientists are:
-
Identifying "protective" microbes that might reduce disease severity
-
Studying how antibiotics, steroids, and antifungals alter the microbiome
-
Investigating faecal or airway microbiota transplants in severe lung disease
-
Developing tests that detect imbalances in lung flora before symptoms worsen
💡 What can you do as a patient?
-
Avoid unnecessary or repeated broad-spectrum antibiotics unless clearly needed
-
Use airway clearance techniques to keep mucus and debris low
-
Ask your clinician if your sputum cultures test for both bacteria and fungi
-
Consider probiotics cautiously, though evidence for lung benefit is still limited
📝 Article 1: What Are Biofilms – And Why Do They Matter in Aspergillosis?
🧫 What is a biofilm?
A biofilm is a protective layer that microorganisms (like fungi and bacteria) create when they stick to a surface — such as the inside of airways, lung cavities, or medical devices. They secrete a sticky matrix of sugars, proteins, and DNA that holds them together and shields them from harm.
In aspergillosis, Aspergillus fumigatus forms biofilms on:
-
Mucus in the lungs
-
Cavities or damaged tissue (e.g. in CPA)
-
Surfaces of bronchial airways, especially in people with asthma or bronchiectasis
Pseudomonas aeruginosa, a bacterium often found alongside Aspergillus, also forms biofilms — and they can even form mixed (dual-species) biofilms together.
❗Why does this matter?
Biofilms protect the microbes inside by:
-
Blocking immune cells from reaching them
-
Preventing antibiotics or antifungals from penetrating the biofilm
-
Allowing microbes to go dormant, then reactivate later
This is one reason why infections in aspergillosis patients can become chronic, relapse frequently, or be very hard to fully clear.
People with CPA, ABPA, SAFS, or fungal bronchitis may experience:
-
Repeated flare-ups or infections despite treatment
-
Persistent coughing, breathlessness, or mucus production
-
Ongoing inflammation in the lungs, even when cultures are negative
🛠 How are biofilms treated?
Current options include:
1. Antifungals and antibiotics
-
Standard antifungals (like voriconazole, posaconazole, isavuconazole) can sometimes penetrate biofilms, but often require longer or higher doses.
-
Inhaled antibiotics (e.g. nebulised colistin or tobramycin) are used in bronchiectasis and can help break into bacterial biofilms.
-
Combined therapy (targeting both bacteria and fungi) may be used in patients with co-infection.
2. Disrupting the biofilm
-
DNase (Pulmozyme) in cystic fibrosis breaks up sticky DNA in mucus where biofilms form.
-
Future treatments aim to use enzymes, surfactants, or nanoparticles to dismantle biofilms.
3. Clearing mucus and infected secretions
-
Chest physiotherapy, postural drainage, and devices like the Acapella® or Flutter® help remove secretions where biofilms sit.
-
Bronchoscopy is occasionally used to clear dense mucus plugs.
🔬 Looking ahead:
Researchers are studying:
-
Drugs that target the biofilm matrix directly
-
Ways to prevent biofilms from forming in the first place
-
New diagnostic tools that detect biofilm presence
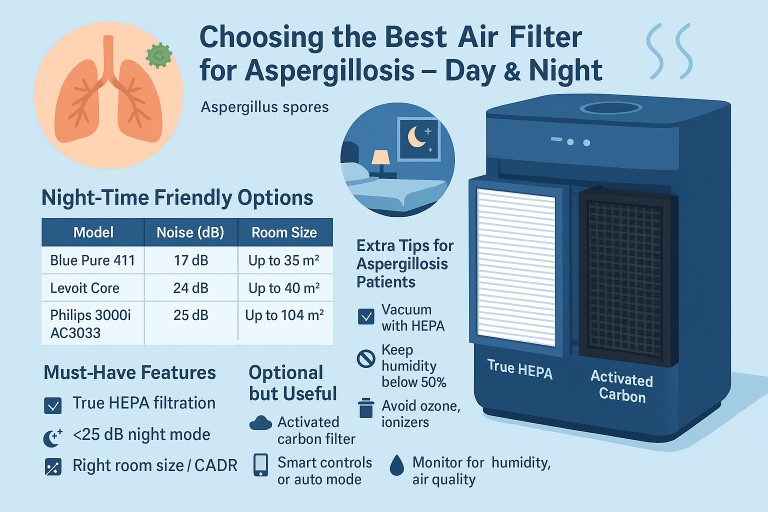
🛡️ Choosing the Best Air Filter for Aspergillosis – Day & Night
Living with aspergillosis (such as ABPA, CPA, aspergillus bronchitis, or SAFS) means taking extra care to avoid airborne Aspergillus spores, which can be found both outdoors and indoors. One of the most effective ways to protect yourself at home is by using a high-quality air purifier.
This guide will help you choose a purifier that works for you — especially for bedroom use at night, where quiet operation is just as important as clean air.
🎯 Why Use an Air Filter?
-
Aspergillus spores are tiny (2–3 microns), invisible to the eye, and can remain airborne for long periods.
-
Indoor sources include dust, damp areas, stored food, compost, or even indoor plants.
-
A HEPA air purifier can trap these particles, helping reduce airway irritation, infections, or allergic reactions.
✅ What to Look For
| Feature | Why It Matters |
|---|---|
| True HEPA Filter | Captures ≥99.97% of particles ≥0.3 microns — includes Aspergillus spores |
| Activated Carbon Filter | Helps remove odours, gases, VOCs (optional bonus) |
| Room Size & CADR | Clean Air Delivery Rate (CADR) should match or exceed your room’s size |
| Quiet Operation | For night-time use, look for ≤25–30 dB (whisper-quiet) |
| Sleep Mode / Dim Lights | Prevents disturbance from lights or fan noise overnight |
| Filter Replacement | Easy to change, ideally with indicator for when to replace |
| No Ozone or Ionisers | Avoids irritation to sensitive lungs — stick with mechanical HEPA filtration |
🌙 Night-Time Friendly Options
| Model | Noise (dB) | Room Size | Notes |
|---|---|---|---|
| Blueair Blue Pure 411 Auto | 17 dB | Up to 35 m² | Super-quiet, ideal for small bedrooms |
| Levoit Core 300S | 24 dB | Up to 40 m² | Quiet, smart controls, affordable |
| Philips 3000i AC3033 | 25 dB | Up to 104 m² | Excellent for larger spaces, smart app |
| IQAir Atem Desk | <22 dB | Personal zone | Ultra-quiet, high-quality for desks/bedsides |
| Dyson Purifier Cool | ~24–32 dB | Medium–large | Stylish, also a fan, more expensive |
Tip: Choose a unit slightly larger than your room size for best effect.
💡 Extra Tips for Aspergillosis Patients
-
✅ Vacuum with a HEPA filter weekly
-
✅ Keep humidity below 50% (use a dehumidifier if needed)
-
✅ Avoid ionizers or ozone generators — these can irritate your lungs
-
✅ Close windows at night during high pollen or spore seasons
-
✅ Clean or change filters regularly (check manufacturer’s guide)
🛏 Night Setup Checklist
-
Place the purifier 1–2 metres from your bed (not right next to your face)
-
Use “Sleep Mode” or low fan for silent overnight cleaning
-
Turn off indicator lights (if bright)
-
Close doors and windows to keep clean air contained
-
Replace filters every 6–12 months or as prompted
📌 Summary
| Must-Have Features | Optional but Useful |
|---|---|
| ✅ True HEPA filtration | 🌫 Activated carbon filter |
| ✅ Quiet night mode (<25 dB) | 📱 Smart controls or auto mode |
| ✅ Right room size / CADR rating | 🌡 Monitor for humidity or air quality |
| ✅ No ozone, no ionizers | 🔁 Filter change indicator |
🗨️ Final Thought
For aspergillosis patients, an air purifier is a worthwhile investment in long-term lung health — especially in sleeping areas where your body is most vulnerable. Choosing the right device helps reduce exposure to fungal spores and improves quality of life, one breath at a time.

📁 Coping with Steroid Side Effects and Finding Balance: A Guide for Aspergillosis Patients
Living with chronic forms of aspergillosis—such as chronic pulmonary aspergillosis (CPA), allergic bronchopulmonary aspergillosis (ABPA), severe asthma with fungal sensitisation (SAFS), or Aspergillus bronchitis—often means taking corticosteroids like prednisolone or hydrocortisone. These powerful medicines can be life-saving, but they also come with physical and emotional side effects, especially at high doses or when taken over long periods.
This guide is here to support you with practical tips, patient stories, and advice on reducing steroids while maintaining your quality of life.
🔊 What Do Steroids Do?
Steroids reduce inflammation and calm overactive immune responses. They're commonly used in aspergillosis to:
- Manage allergic reactions (e.g. in ABPA)
- Control lung inflammation
- Treat adrenal insufficiency or steroid withdrawal symptoms
🔁 Why Reducing Steroids Can Be So Difficult
Steroids are very effective but also powerful. Tapering the dose can cause:
- Return of pain, fatigue, breathing problems, or inflammation
- Steroid withdrawal symptoms (fatigue, low mood, joint pain)
- Adrenal suppression if the body has stopped making its own cortisol
Many patients report:
“I reduced by 1mg and everything fell apart.” “I want to be on less, but life is unbearable when I try.”
You are not failing. Finding the right dose is a balance between lowering risks and keeping your life manageable.
🛋 Common Side Effects and What You Can Do
| Side Effect | Tips to Cope |
|---|---|
| Increased appetite | Plan balanced meals, high-fibre snacks, drink water, be kind to yourself |
| Weight gain / swelling | Gentle movement, reduce salt, try pressotherapy (discuss with your team) |
| Mood swings or anxiety | Talk about it, track your feelings, ask about counselling or peer support |
| Insomnia | Avoid caffeine late, consider timing of dose, try a calming bedtime routine |
| "Moon face" / puffiness | Often fades when dose is reduced; hydrate and moisturise |
| Muscle/joint pain or weakness | Gentle stretches, walking, low-impact activity, speak to a physio if needed |
| Bruising/thin skin | Moisturise, protect from bumps, avoid strong detergents |
| Raised blood sugar | Eat regularly, reduce sugary drinks, ask about monitoring if concerned |
| Bone thinning | Ask about calcium, vitamin D, or bone-protecting medications |
| Adrenal suppression | Never stop suddenly; always taper with a doctor's guidance |
👥 Real Patient Stories and Analogies
🐻 Alison's Bears
“There are two bears inside me. Prednisone Bear is wild and wants to eat and sleep and snap. But Rusty McTravel Bear is my real self—gentle, curious, slowly trying to get back on the road. I’ve learned to recognise the first and nurture the second.”
🏎️ The Revving Car
“Being on steroids sometimes feels like a car with the engine revving but the brakes on. You’re buzzing, but you’re stuck. Try easing the brakes: take a walk, make tea, do something simple to use the energy.”
🚩 Finding Your Balance: When Less Isn't Always Better
✅ Go slow
- Taper in small steps—as little as 0.5–1mg at a time
- Wait several weeks between reductions
✅ Keep a steroid diary
- Note dose, mood, sleep, symptoms, activity
- This helps identify your "minimum effective dose"
✅ Accept that a small maintenance dose may be necessary
- You are not failing if you need 2mg, 5mg, or 7.5mg long-term
- The goal is a life worth living, not perfection
✅ Ask about alternatives
- Inhaled steroids, antifungals, or biologics might help reduce systemic steroid use
✅ Consider adrenal testing
- Especially if you feel unwell during tapering or on low doses
🛏️ Other Strategies That May Help
- Pressotherapy for leg pain and swelling
- Mindfulness or breathing exercises for anxiety or insomnia
- Peer support (online or in person)
- Short-term plans: some patients use a "rescue dose" plan for flare-ups
- Talk to your care team: never reduce on your own without guidance
💼 Summary
Reducing or living with steroids is not just about doses. It’s about protecting your body and your sense of self. If a small daily dose keeps you functioning, that is not weakness—it’s balance.
You are not alone. Many in the aspergillosis community are navigating this same path.
“The right dose is the one where I can breathe, move, smile — and still feel like myself.”
🛡️ Staying Safe with Self-Treatment and Complementary Therapies: A Guide for Aspergillosis Patients
Living with a chronic condition like aspergillosis — whether chronic pulmonary aspergillosis (CPA), allergic bronchopulmonary aspergillosis (ABPA), severe asthma with fungal sensitisation (SAFS), or aspergillus bronchitis — can be exhausting. Many patients explore over-the-counter (OTC) products, natural remedies, or complementary therapies to gain a sense of control.
But how can you be sure a product or therapy is safe, effective, and not a waste of money?
This guide aims to help.
🔍 Why Do Patients Try Things on Their Own?
In many countries, it’s common to self-medicate or explore alternative treatments without consulting a healthcare professional. Reasons include:
-
Limited access to specialist care
-
Cultural norms that favour self-management
-
Easy access to remedies and supplements online or in shops
-
Feeling unheard or unsupported in mainstream medical care
Even in the UK, patients with aspergillosis may turn to:
-
Herbal products
-
Nutritional supplements
-
Creams or gels with capsaicin (chilli), turmeric, or menthol
-
Breathing techniques, steam inhalation
-
“Immune-boosting” diets or over-the-counter fungal cleanses
Some of these may be helpful — but not all are safe or worthwhile.
✅ Step 1: How to Check if a Product or Therapy Is Safe
Before trying anything new, ask:
1. Is it approved or regulated in the UK?
Medicines and certain creams should have a Product Licence (PL) number, issued by the Medicines and Healthcare products Regulatory Agency (MHRA).
You can check the licence on the MHRA product registry.
2. Could it interact with your prescribed medications?
-
Some herbal remedies affect azole antifungal drugs (like itraconazole or voriconazole) or oral steroids.
-
Ask your GP (General Practitioner), specialist, or pharmacist before combining treatments.
3. Is it safe to apply or inhale?
-
Never use essential oils, menthol, or herbal mixtures in a nebuliser unless clearly intended for lung use.
-
Avoid applying hot or irritating creams to broken or sensitive skin.
4. Is it mentioned in NHS guidance?
Stick to advice on:
-
Your local hospital trust’s respiratory or infectious disease guidelines
-
National Institute for Health and Care Excellence (NICE) recommendations
-
Cochrane Reviews or published clinical trials
⚠️ Watch Out for Red Flags
Be cautious of any product, practitioner, or website that:
| 🚩 Red Flag | ⚠️ Why It’s a Concern |
|---|---|
| Claims to “cure” aspergillosis | There is no cure — only long-term management |
| Says it’s “100% natural with no side effects” | Natural products can still be harmful |
| Uses high-pressure sales tactics | Legitimate care is never urgent or fear-based |
| Recommends stopping your prescribed treatment | Stopping antifungals or steroids can be dangerous |
🧪 Step 2: Look for Evidence, Not Just Testimonials
Some treatments are promising — but we need solid evidence to know they work.
✅ Good sources of trustworthy evidence:
-
Cochrane Library (systematic reviews of healthcare studies)
-
Electronic Medicines Compendium (EMC): www.medicines.org.uk
-
NHS Trust guidelines or clinical leaflets
-
Published studies on PubMed, ClinicalTrials.gov, or from recognised research institutions
💬 Can You Trust a Pharmacist?
Yes — in most cases, UK pharmacists are highly trained and regulated. However, there are two kinds to be aware of:
| Type of Pharmacist | What to Know |
|---|---|
| Retail Pharmacist | May sell you products directly; still bound by safety standards |
| Clinical Pharmacist (in GP surgeries or hospitals) | Focused entirely on clinical care and not sales-driven |
Both are regulated by the General Pharmaceutical Council (GPhC) and must put patient safety first, regardless of sales.
🟢 Ask them:
-
“Will this interact with my medications?”
-
“Is this supported by NHS or NICE?”
-
“Would this be suitable for someone with CPA or ABPA?”
🧘 What About Complementary Therapies?
Some patients explore:
-
Acupuncture
-
Herbal medicine
-
Osteopathy or chiropractic
-
Reflexology or massage
-
Nutritional therapy
-
Mindfulness and yoga
These may help with:
-
Muscle or joint pain
-
Fatigue and sleep problems
-
Emotional stress or anxiety
They can complement your medical treatment — but should never replace it.
✅ Safe if:
-
Practitioner is registered with a reputable UK body
-
The therapy does not interfere with prescribed medications
-
It is used for symptom relief, not for “cleansing” or treating the infection
❌ Risky if:
-
It’s marketed as a cure for aspergillosis
-
It encourages you to stop medical treatment
-
It is expensive, secretive, or vague about its effects
Reputable UK Registers:
| Practitioner Type | Regulator / Body |
|---|---|
| Acupuncturists | British Acupuncture Council (BAcC) |
| Herbalists | National Institute of Medical Herbalists (NIMH) |
| Osteopaths | General Osteopathic Council (GOsC) |
| Chiropractors | General Chiropractic Council (GCC) |
| Nutritionists | Association for Nutrition (AfN) |
🧾 Summary: A Safer Way to Explore New Treatments
| ✅ Do This | ❌ Avoid This |
|---|---|
| Check the MHRA or NHS website | Trusting social media or forums alone |
| Look for a PL number and regulated status | Using unlicensed creams, drops, or nebuliser fluids |
| Ask your pharmacist or GP about interactions | Assuming “natural” means harmless |
| Use one new treatment at a time | Trying multiple new remedies together |
| Start with low doses or small trial sessions | Buying expensive long-term “packages” up front |
📘 Real Example: Using Capsaicin Cream for Pain
Some patients with back pain or joint discomfort have tried capsaicin cream (chilli-based), especially if they cannot tolerate non-steroidal anti-inflammatory drugs (NSAIDs) like ibuprofen.
✅ It’s safe for many people when:
-
Applied in small amounts to intact skin
-
Hands are washed after use
-
Used up to 4 times daily
-
Product is licensed (e.g. Zacin® 0.025%)
⚠️ It may cause a burning feeling for the first few days.
Avoid contact with eyes, mouth, or mucous membranes.
Ask a pharmacist before use — especially if you’re on steroids, have skin thinning, or are very sensitive to heat or irritation.
🗂️ Want to Learn More?
-
Visit www.aspergillosis.org
-
Contact the National Aspergillosis Centre (NAC) in Manchester
-
Speak to your GP or hospital respiratory specialist
-
Ask in trusted support groups like the Aspergillosis Support Facebook Group

🌿 Living Well with Aspergillosis: Understanding the Role of Palliative Care
Many people think palliative care is only for those at the very end of life. But that’s a common misconception — especially for people living with aspergillosis, including chronic pulmonary aspergillosis (CPA), ABPA, or aspergillus bronchitis.
Palliative care is not about giving up. It’s about living better, with more comfort, dignity, and control — no matter how far along you are in your illness.
💬 What Is Palliative Care?
Palliative care is specialist medical support for people with serious, long-term, or life-limiting illnesses. It focuses on:
-
Managing symptoms like pain, breathlessness, or fatigue
-
Providing emotional and psychological support
-
Helping you plan ahead for the future
-
Supporting families and carers
✅ It can be given alongside antifungal or active treatments and is not limited to the last weeks or months of life.
🌟 How Can It Help People with Aspergillosis?
People living with aspergillosis often face unpredictable flare-ups, side effects from long-term treatment, hospital admissions, and emotional strain. Palliative care can help with:
✅ 1. Symptom Control
Manage persistent symptoms such as:
-
Breathlessness
-
Chest pain or discomfort
-
Coughing
-
Fatigue
-
Side effects from antifungal or steroid use
✅ 2. Emotional and Mental Health Support
Chronic illness can lead to anxiety, depression, or fear of decline. Palliative teams include trained counsellors and therapists.
✅ 3. Practical Support
Physiotherapists, occupational therapists, and social workers can help with equipment, managing daily tasks, and staying independent.
✅ 4. Family and Carer Support
Caring for someone with aspergillosis can be exhausting and emotionally tough. Palliative care includes carer support, respite advice, and bereavement services.
✅ 5. Planning Ahead
Advance care planning helps you express your wishes for future treatment, care, or emergencies — so your preferences are known and respected.
🧭 Who Can Receive Palliative Care?
Anyone with serious symptoms, emotional distress, or planning needs related to a chronic or progressive illness — even if you’re still on active treatment.
✅ Core criteria include:
-
Ongoing symptoms that are hard to control
-
Emotional or psychological distress
-
Progressive disease or declining health
-
Complex care needs for you or your family
-
Multiple hospital admissions or infections
Tools like the Supportive and Palliative Care Indicators Tool (SPICT) or your GP's Gold Standards Framework register may be used to support a referral, but your experience matters most.
❌ What If You’re Told “You’re Not Ready”?
If you’re told, “you’re not ready for palliative care yet,” remember:
-
Needing help now means you’re ready.
-
Palliative care is about quality of life — not prognosis.
-
It’s common for healthcare professionals to associate palliative care only with end-of-life, but that’s outdated thinking.
💬 What to Say
If dismissed, try:
“I understand palliative care is about improving quality of life at any stage. I’d really value support now with symptoms and planning ahead.”
Or:
“I’m not asking to stop treatment. I want help managing the impact this illness is having on my life.”
If needed, request a second opinion or contact your local hospice directly. Many offer advice even without a referral.
🕰️ When Should I Ask for Palliative Care?
The best time is as early as you feel you need extra support. Don't wait for a crisis.
Research shows that early palliative care:
-
Improves quality of life
-
Reduces hospital visits
-
Can even extend life in some cases
-
Helps you and your loved ones feel more in control
📞 How to Access Palliative Care
| Step | What to Do |
|---|---|
| 1. Talk to your GP or hospital team | Ask if there’s a palliative care or community team you can speak to. You don’t need to be near the end of life. |
| 2. Ask about local services | Find out if there’s a hospice outreach nurse, home visits, or symptom clinic nearby. |
| 3. Contact a hospice directly | Many offer support to people with respiratory conditions, even if you're not staying with them. |
| 4. Ask for a holistic needs assessment | You're entitled to one after being diagnosed with a serious or long-term condition. It can highlight unmet needs. |
| 5. Reach out to charities and support lines | See below for trusted sources of advice and emotional support. |
🧭 Useful Contacts and Resources
-
Marie Curie Support Line: 0800 090 2309 – Emotional and practical advice
-
Macmillan Cancer Support: 0808 808 0000 – Also helps with non-cancer conditions like chronic lung disease
-
Hospice UK Directory: www.hospiceuk.org – Find your local hospice
-
NHS Website: www.nhs.uk – Search “palliative care” for general information
-
Compassion in Dying: www.compassionindying.org.uk – Advance care planning resources
💬 Final Thought
Palliative care is not about giving up — it’s about living well with support. For aspergillosis patients facing ongoing symptoms, uncertainty, or stress, this kind of care can be transformative.
📢 You have the right to ask for help. Don’t wait until someone tells you it’s time — the right time is when you feel you need it.