Biologics are modern injection or infusion treatments that target the immune system. They can help people with Allergic Bronchopulmonary Aspergillosis (ABPA) by reducing inflammation, cutting down on steroid use, and lowering flare-ups.
In the UK, consultants must follow NICE (National Institute for Health and Care Excellence) guidance, which sets both clinical criteria and cost-effectiveness rules.
🔎 Step 1: Who qualifies?
-
You must already be on high-dose inhalers and still have severe symptoms.
-
Decisions are made by a specialist severe asthma / ABPA clinic team (MDT).
-
Blood tests, flare history, and steroid use are all considered.
🧭 Step 2: Which biologic?
Consultants match the drug to the type of inflammation you have:
| Pathway / Clues | Possible Biologic | Notes |
|---|---|---|
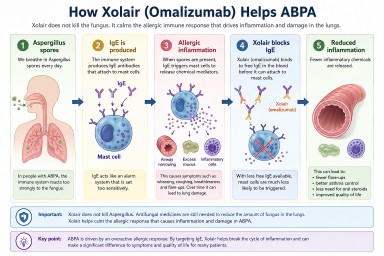
| IgE-allergic (allergic tests positive, high IgE) | Omalizumab (Xolair) | Works best if perennial allergies are driving symptoms. |
| Eosinophilic (high eosinophil counts, frequent flare-ups, or long-term steroid use) | Mepolizumab (Nucala) or Benralizumab (Fasenra) | NHS requires doctors to choose the least-expensive if both fit. |
| Eosinophils ≥400 + frequent flare-ups | Reslizumab (Cinqaero, IV drip) | Less used, but an option if IV therapy is acceptable. |
| Still severe after above / not eligible | Dupilumab (Dupixent) | Also helps if you have eczema or nasal polyps. |
| Any type, severe with ≥3 flare-ups or on daily steroids | Tezepelumab (Tezspire) | Works even if blood tests don’t show high eosinophils or IgE. |
🛑 Step 3: Stop if no benefit
NICE requires a 12-month review.
-
If your flare-ups or daily steroid dose haven’t fallen enough (usually by ≥50%), treatment should stop.
💷 Why cost matters
-
The NHS only funds biologics judged “cost-effective.”
-
If two drugs are equally suitable, consultants must use the least-expensive one.
-
This doesn’t mean you won’t get the right drug — but sometimes doctors must justify why one biologic is better for you personally.
📌 What this means for ABPA patients
-
ABPA is not directly covered by NICE guidance, but the same biologics are often used if you also meet asthma criteria.
-
Main goals:
-
Reduce oral steroids (prednisolone) and their side-effects.
-
Control flare-ups and lung damage.
-
-
Evidence supports omalizumab, mepolizumab, benralizumab, and dupilumab in ABPA; tezepelumab has less data so far.
✅ Bottom line:
Biologics can be life-changing for ABPA patients, but the NHS pathway means the choice depends on your blood results, flare history, steroid needs — and cost-efficiency rules. If one option doesn’t work, another may still be possible.