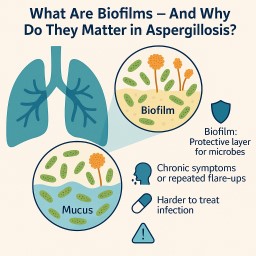
🧫 What is a biofilm? A…
by GAtherton
Sadly, at the time of writing…
1. 🌡 What Is Haemoptysis?…
If you’ve finished a course…
If you're being treated for…
There are no classic…
🔹 Sometimes, yes — but it…