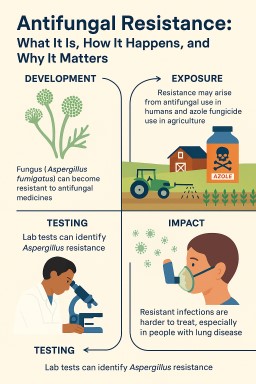
Antifungals

Medicine Leaflets, Side Effects, and Interactions: Where to Find Reliable Information
When you open a new box of…

Side Effects, New Medicines, and Safety Reporting: What Every Patient Should Know
Modern medicines, including…

Working With Your Medical Team: What Every Patient With Aspergillosis Needs to Know
Modern antifungal treatments,…
🦠 Understanding Antibiotic Use in Aspergillosis: A Guide to Antimicrobial Stewardship (AMS)
This information is provided…



💊 General Strategies to Reduce Antimicrobial Resistance in Clinical Practice
1. IV to Oral Switch (IVOS)…