Browse information
Latest Articles
Support
For Professionals
Search
Complications
Home
Archive by Category "Complications"
Complications
Are all your medicines still helping? A guide to polypharmacy and medication reviews
by GAtherton
NTM and aspergillosis: why are they increasingly found together?
by GAtherton
Understanding Antibiotics: A Guide for People Living with Aspergillosis and Bronchiectasis
by GAtherton
Loosen and Clear Mucus: Practical Self-Help Techniques for People with Aspergillosis
by GAtherton
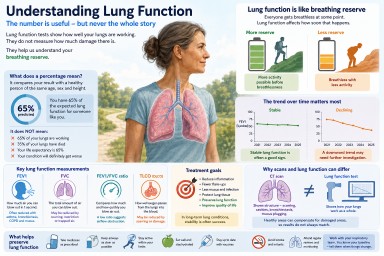
Understanding Lung Function in Aspergillosis and Asthma
by GAtherton
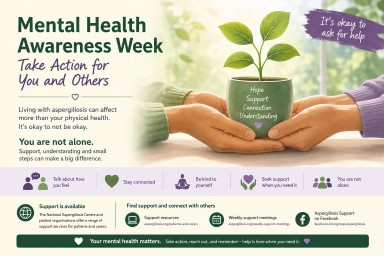
Mental Health Awareness Week: Supporting the Emotional Impact of Aspergillosis
by GAtherton
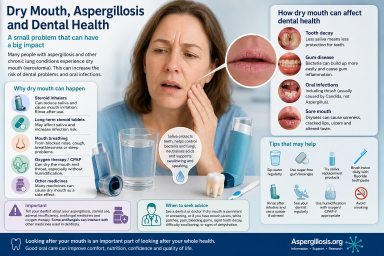
Dry Mouth, Aspergillosis and Dental Health
by GAtherton
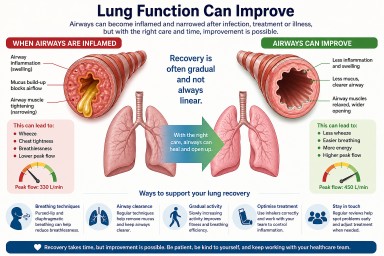
Can Lung Function Improve After Infection or Treatment?
by GAtherton
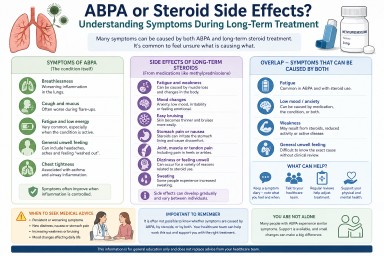
ABPA or Steroid Side Effects? Understanding Symptoms During Long-Term Treatment
by GAtherton
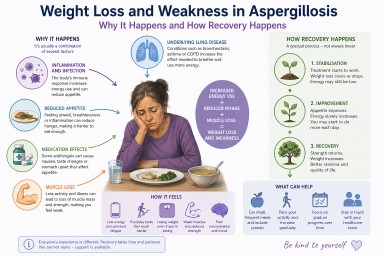
Weight Loss and Weakness in Aspergillosis: Why It Happens, How It Feels, and What Helps Recovery
by GAtherton
1
2
3
4