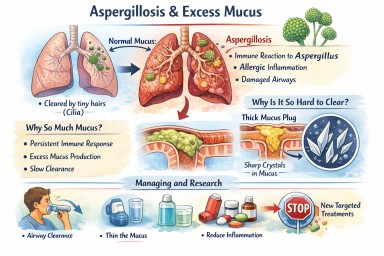
How fungal spores interact…
by GAtherton
Many people with…
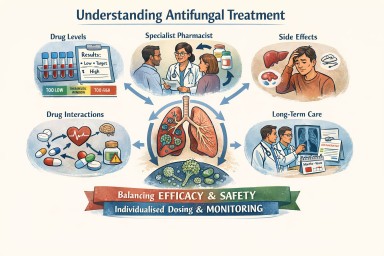
A detailed reference for…
A clear, patient-friendly…
Why adrenal insufficiency can…
1. What exactly is a……
People living with…
A Complete Patient Guide**…
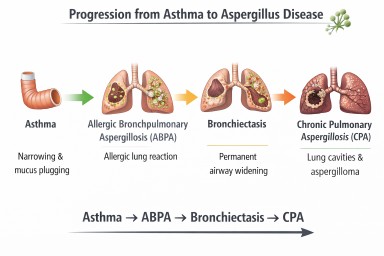
You may have read headlines…
Many patients with ABPA,…