Complications
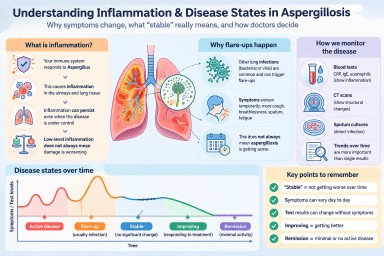
Inflammation and Aspergillosis: Understanding “Stable”, “Flare”, and “Improving” Disease
Last reviewed: April 2026…

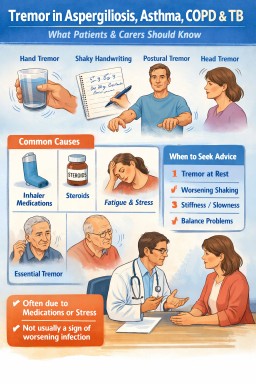
Muscle Cramps in Aspergillosis (Including ABPA and CPA): Causes, Triggers, and What May Help
Last reviewed: March 2026…
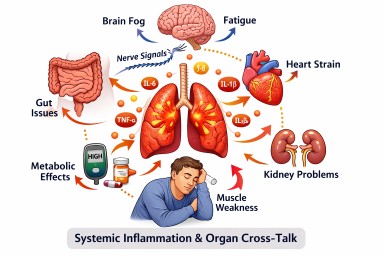
How Inflammation in One Part of the Body Can Affect the Rest of the Body
Last reviewed: 24 March 2026…

Managing fatigue and energy in aspergillosis and allergic fungal lung disease
Key points Many people with…