Antibiotics are among the most important medicines used to treat bacterial infections, yet many people living with aspergillosis and bronchiectasis receive repeated courses without ever having their purpose fully explained. This guide explains why antibiotics are prescribed, how doctors choose them, why resistance matters, what side effects and interactions to watch for, and how future treatments may become faster and more precise.
Key points
- Antibiotics treat bacterial infections. They do not treat Aspergillus, which is a fungus.
- Many people with aspergillosis also have bronchiectasis, asthma, COPD or damaged airways, making bacterial infections more likely.
- The “strongest” antibiotic is not always the best choice. Doctors usually aim to use the antibiotic that is most likely to work while causing the least unnecessary harm.
- Sputum samples help identify which bacteria are present and which antibiotics are likely to work.
- Antibiotic resistance develops in bacteria, not in people.
- Side effects, allergies, kidney and liver function, and drug interactions all influence antibiotic choice.
- People taking antifungal medicines should always tell their doctor or pharmacist before starting antibiotics.
- The future of infection treatment is likely to involve faster diagnostics, more targeted antibiotics, sequencing, AI, vaccines and other precision approaches.
1. Why this guide?
Many people living with aspergillosis are prescribed antibiotics at some point. Some receive occasional short courses, while others need antibiotics repeatedly because they also have bronchiectasis, COPD, asthma, recurrent chest infections or other lung conditions.
Many patients tell us that they have taken antibiotics for years but have never had the opportunity to understand why different antibiotics are chosen, why some are changed, why others are avoided, or how these decisions are made. This guide aims to answer those questions.
Antibiotics can be very important medicines. They can treat bacterial infections, prevent serious complications and help people recover from a worsening chest condition. However, they can also cause side effects, interact with other medicines, disturb the microbiome and contribute to antibiotic resistance if they are used when they are not needed.
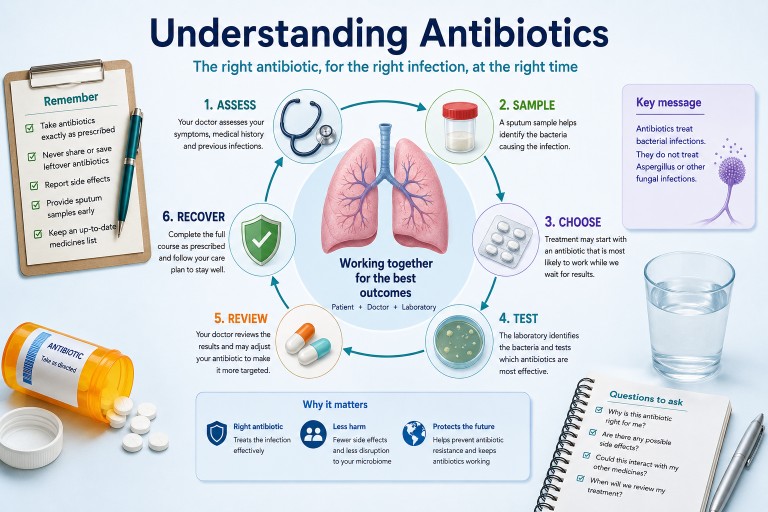
Key message
Antibiotics treat bacterial infections. They do not treat Aspergillus itself. Aspergillosis is caused by a fungus and requires antifungal treatment when active treatment is needed.
The aim of this guide is not to help people choose antibiotics for themselves. Antibiotics should always be prescribed by a qualified healthcare professional who understands your medical history, test results, allergies, current medicines and local prescribing guidance.
Instead, this guide aims to help you have better conversations with your healthcare team. Understanding why decisions are made can make treatment feel less confusing and help you share information that may be important, such as previous sputum results, antibiotics that have helped before, side effects you have experienced, or medicines that might interact.
If you are unwell, coughing up blood, becoming more breathless, developing chest pain, confused, drowsy, feverish or rapidly deteriorating, seek urgent medical advice. This guide is for general education and should not replace individual medical care.
2. Why do people with aspergillosis need antibiotics?
One of the most common questions people ask is:
“If aspergillosis is caused by a fungus, why am I taking antibiotics?”
The answer is that many people living with aspergillosis also develop bacterial chest infections. These infections require antibiotics because antibiotics treat bacteria, not fungi.
Although aspergillosis itself is caused by the Aspergillus fungus, it often occurs alongside other lung conditions that make bacterial infections more likely. This means it is not unusual for someone to receive antifungal medication at one time and antibiotics at another, or occasionally both at the same time.
Bacteria, fungi and viruses: what is the difference?
| Type of germ | Examples | Usual treatment approach |
|---|---|---|
| Bacteria | Many chest infections, Haemophilus influenzae, Pseudomonas aeruginosa, Streptococcus pneumoniae | Antibiotics |
| Fungi | Aspergillus, Candida | Antifungal medicines |
| Viruses | Influenza, COVID-19, RSV and many common colds | Usually supportive care, with antiviral medicines for some infections |
This distinction is important because antibiotics do not kill fungi or viruses. Taking an antibiotic will not treat aspergillosis itself.
Why are bacterial infections more common in some people with aspergillosis?
Many people with aspergillosis also have underlying lung conditions that make it easier for bacteria to grow.
Bronchiectasis is a common example. It causes widening and damage to the airways, making it harder for the lungs to clear mucus effectively. When mucus remains in the lungs, bacteria have more opportunity to multiply and cause infection.
Other conditions, such as severe asthma or COPD, can also affect the lungs’ natural defence mechanisms. Previous lung damage, surgery or repeated infections may further increase the risk.
Some medicines used to control inflammation, including corticosteroids, can also reduce the body’s ability to fight infection, although they are often essential parts of treatment.
Can more than one problem happen at the same time?
Yes. This is one reason chest symptoms can be difficult to diagnose and treat.
A person may have:
- aspergillosis that is stable, but a new bacterial chest infection;
- worsening aspergillosis without any bacteria being involved;
- a viral infection that triggers worsening respiratory symptoms;
- or a combination of bacterial, fungal and viral problems occurring together.
Because many of these illnesses produce similar symptoms, including cough, increased sputum, breathlessness and tiredness, your healthcare team may need sputum samples, blood tests or scans to determine what is happening.
Not every flare-up needs antibiotics
When symptoms worsen, it is natural to think that antibiotics are needed. However, this is not always the case.
Breathlessness, increased cough or fatigue may be caused by a bacterial infection, but they may also be caused by a viral infection, a flare-up of aspergillosis, airway inflammation, asthma, allergy or another medical condition.
Choosing the right treatment begins with understanding what is causing the symptoms, rather than simply treating the symptoms themselves.
3. How do doctors decide which antibiotic to prescribe?
Many people are surprised by how much thought goes into choosing an antibiotic. Although several antibiotics may be able to treat the same infection, the best choice depends on much more than simply identifying the bacteria.
Your healthcare professional has to balance a number of factors to select an antibiotic that is both effective and safe for you.
What information does your doctor consider?
Before prescribing an antibiotic, your healthcare team may consider:
- your symptoms and how severe they are;
- whether the infection is likely to be bacterial, viral or fungal;
- your underlying lung conditions, such as bronchiectasis, asthma or COPD;
- previous sputum culture results;
- which bacteria have caused infections in the past;
- which antibiotics have worked well previously;
- which antibiotics have not helped, or have caused side effects;
- any antibiotic allergies;
- your kidney and liver function;
- other medicines you are taking that could interact;
- local antibiotic resistance patterns;
- whether treatment is needed at home or in hospital.
Sometimes doctors have to make their best judgement
Ideally, doctors would know exactly which bacterium is causing an infection before treatment begins. Unfortunately, laboratory cultures usually take at least a day or two, and sometimes longer.
If someone is becoming unwell, waiting several days may not be safe.
Instead, doctors often begin empirical treatment. This means prescribing the antibiotic that is most likely to work based on your symptoms, the bacteria that commonly cause similar infections, your previous microbiology results and local knowledge of antibiotic resistance.
Once sputum culture or other laboratory results become available, treatment can be reviewed. Sometimes the original antibiotic is continued because it is working well. At other times it may be changed to one that is more specifically targeted to the bacteria that have been identified.
Did you know?
Many people start antibiotic treatment before laboratory results are available. This is common medical practice and helps ensure that serious infections are treated promptly while additional information is being collected.
Why don’t two patients receive the same antibiotic?
Two people with similar symptoms may receive different antibiotics.
For example, one person may have previously grown Pseudomonas aeruginosa in their sputum, while another has repeatedly grown Haemophilus influenzae. One may have a penicillin allergy, another may have reduced kidney function, while a third may be taking medicines that interact with certain antibiotics.
The most appropriate antibiotic is therefore highly individual.
Previous infections matter
Your previous microbiology results are often one of the most valuable pieces of information available.
If you have had repeated infections with the same bacterium, your healthcare team may already know which antibiotics usually work well, which have failed previously, whether resistance has developed, and whether your bacteria have become more difficult to treat over time.
This is one reason why specialist clinics often ask about previous sputum results when reviewing your treatment.
4. Broad-spectrum and narrow-spectrum antibiotics
One of the most common misunderstandings about antibiotics is that some are “strong” while others are “weak”. In reality, doctors usually think in terms of broad-spectrum and narrow-spectrum antibiotics rather than strength.
The aim is not to prescribe the most powerful antibiotic available. Instead, it is to choose the antibiotic that is most likely to treat your infection while causing the least unnecessary harm.
What does “broad-spectrum” mean?
Broad-spectrum antibiotics are active against a wide range of different bacteria.
They are particularly useful when the exact bacterium is not yet known, several different bacteria could be responsible, or the infection is serious and treatment cannot safely wait for laboratory results.
Because they affect many different bacteria, broad-spectrum antibiotics may also disturb the body’s normal bacteria more than a narrower-spectrum antibiotic.
What does “narrow-spectrum” mean?
Narrow-spectrum antibiotics are designed to treat a smaller range of bacteria.
Once laboratory tests identify the bacterium causing an infection, doctors often prefer to use a narrow-spectrum antibiotic whenever possible.
This approach helps to treat the infection effectively, reduce unnecessary exposure to antibiotics, protect the body’s normal bacteria and slow the development of antibiotic resistance.
Think of it like gardening
A broad-spectrum antibiotic is a little like using a weedkiller that kills almost every plant in a flower bed. It may solve the immediate problem, but it can also affect plants you wanted to keep.
A narrow-spectrum antibiotic is more like carefully removing only the weed causing the problem. It is a more targeted approach that leaves the surrounding plants largely undisturbed.
Examples of antibiotics commonly used for chest infections
There are many different antibiotics available, and the choice depends on the type of infection, the bacteria involved, previous sputum culture results, allergies, side effects, other medicines you are taking and local prescribing guidance.
The examples below illustrate some antibiotics that people with chronic lung conditions may encounter. They are included to help explain how doctors think about antibiotic selection, not to suggest that one antibiotic is better than another.
| Antibiotic | Common respiratory uses | Spectrum* | Things patients should know |
|---|---|---|---|
| Amoxicillin | Common bacterial chest infections | Relatively narrow | Often an excellent first-choice antibiotic when the likely bacteria are susceptible. |
| Co-amoxiclav | A wider range of respiratory infections | Broad | Covers more bacteria than amoxicillin alone but may cause more digestive side effects in some people. |
| Doxycycline | Many respiratory infections, particularly when penicillin is unsuitable | Broad | Can cause photosensitivity, making skin more sensitive to sunlight. |
| Azithromycin | Long-term prevention of exacerbations in selected people with bronchiectasis | Relatively narrow | Often prescribed for its anti-inflammatory effects as well as its antibacterial activity. It is not suitable for everyone and requires careful monitoring. |
| Ciprofloxacin | Often used when bacteria such as Pseudomonas aeruginosa are present and susceptible | Broad | Usually reserved for specific situations because of concerns about resistance and potentially important side effects. |
*Spectrum is a simplified description. Some antibiotics do not fit neatly into “broad” or “narrow” categories, and the best antibiotic depends on the individual patient and the bacteria causing the infection.
Did you know?
There are many licensed antibiotics, but only a relatively small number are used routinely for most community chest infections. Others are reserved for specific bacteria, resistant infections or hospital use. Protecting these specialist antibiotics is an important part of antimicrobial stewardship.
Why not always prescribe the broadest antibiotic?
It might seem logical to use the antibiotic that kills the greatest number of bacteria, but this is not usually the best approach.
Using unnecessarily broad antibiotics can increase the risk of antibiotic resistance, cause more side effects, disturb the normal bacteria living in the gut and elsewhere in the body, increase the risk of infections such as Clostridioides difficile (C. difficile), and reduce future treatment options if resistant bacteria develop.
For these reasons, doctors aim to use the narrowest effective antibiotic whenever it is safe to do so.
Remember
Doctors do not usually ask, “Which is the strongest antibiotic?” Instead they ask, “Which antibiotic is most likely to treat this infection safely and effectively while causing the least unnecessary harm?”
Can treatment change once test results are available?
Yes. It is quite common for doctors to begin treatment with a broader-spectrum antibiotic while waiting for sputum culture results. Once the laboratory identifies the bacterium and reports which antibiotics are likely to work, treatment may be changed to a more targeted medicine.
This process is known as stepping down or de-escalating antibiotic treatment. It is an important part of good antimicrobial stewardship and helps preserve antibiotics for the future.
5. Why have I been prescribed an antibiotic that didn’t seem to work before?
Many people living with bronchiectasis or aspergillosis have experienced repeated chest infections over many years. It is not unusual to be prescribed the same antibiotic more than once.
This can be frustrating, especially if you remember taking that antibiotic previously and feeling that it made little difference.
“I’ve had this antibiotic before. It never works.”
Although this is an understandable reaction, the situation is often more complicated than it first appears.
The infection may not be the same
Not every chest infection is caused by the same bacterium.
One episode may be caused by one type of bacteria, while the next may involve a completely different organism. Sometimes symptoms are caused by a viral infection, worsening aspergillosis, inflammation or another lung condition rather than bacteria at all.
An antibiotic that was appropriate for one illness may therefore be less suitable for another, or the other way around.
The previous illness may not have been bacterial
Antibiotics only work against bacteria.
If your previous symptoms were caused by a virus, a flare-up of aspergillosis, airway inflammation or another non-bacterial cause, then no antibiotic would have been expected to help very much, regardless of which one was prescribed.
This does not necessarily mean the antibiotic itself was ineffective.
Your doctor may have different information this time
Each consultation is slightly different.
Your doctor may now know which bacteria have previously grown in your sputum, which antibiotics those bacteria were sensitive to, whether resistance has developed, whether you have new medical conditions, or whether your current medicines have changed.
Even if the same antibiotic is prescribed, the decision may be based on new information.
A new doctor may not know your previous experience
If you are seen by an out-of-hours service, an emergency department or a clinician who does not usually look after you, they may not immediately have access to your full treatment history.
They may know that you have a chest infection but not which antibiotics have helped, failed or caused side effects in the past.
Helping your healthcare team
Instead of simply saying, “That antibiotic never works,” it is often more helpful to explain when you last received it, whether you completed the course, whether your symptoms improved at all, whether another antibiotic was eventually needed, whether a sputum sample identified a particular bacterium, and whether you experienced any important side effects.
Sometimes the antibiotic really was not the right one
Doctors are not always able to identify the exact cause of an infection before treatment begins.
Initial antibiotic treatment is often based on experience and the bacteria most likely to be responsible. Occasionally, laboratory results later show that a different antibiotic would be more appropriate.
Changing antibiotics after sputum culture results become available is common and should not be seen as a failure. Instead, it reflects the fact that treatment is being refined as more information becomes available.
Good communication improves future treatment
If you experience repeated chest infections, keeping a simple record of your treatment history can be extremely helpful.
You may wish to note the date of each infection, whether a sputum sample was taken, which bacteria were identified, which antibiotic was prescribed, whether it appeared to help, and any significant side effects.
Many patients find that this information becomes particularly valuable during hospital admissions, emergency appointments or consultations with new healthcare professionals.
6. Why are sputum samples so important?
If you live with bronchiectasis or aspergillosis, your healthcare team may ask you to provide a sputum sample whenever your symptoms worsen.
This can feel inconvenient, particularly if you are coughing more or feel unwell. However, a good sputum sample is often one of the most valuable tools available for identifying the cause of a chest infection and selecting the most appropriate treatment.
What is a sputum sample?
Sputum is the mucus that is coughed up from deep within the lungs. It is different from saliva, which is produced in the mouth.
Because sputum comes from the lower airways, it can contain bacteria, fungi and other organisms that are living in or causing infection within the lungs.
Key message
A sputum sample helps your healthcare team identify what is causing an infection rather than relying only on an educated guess.
What happens to my sample?
Once your sputum reaches the microbiology laboratory, several different tests may be performed depending on your symptoms and medical history.
These may include looking for bacteria that commonly cause chest infections, identifying fungi such as Aspergillus where appropriate, testing which antibiotics are most likely to work against any bacteria that are found, and, in some situations, carrying out specialised molecular tests.
Not every sample receives every test. The investigations performed depend on the clinical information provided by your healthcare team.
What is a culture?
One of the most common laboratory tests is called a culture.
During a culture, the laboratory attempts to grow bacteria or fungi from your sputum under carefully controlled conditions. If organisms grow, they can often be identified and tested against different antibiotics to determine which treatments are most likely to be effective.
This process takes time, which is why laboratory results are usually not available immediately.
What is antibiotic susceptibility testing?
Finding a bacterium is only part of the story.
The laboratory also wants to know which antibiotics are likely to stop it growing.
This process, known as antibiotic susceptibility testing, helps doctors move from an educated guess to a more targeted treatment plan.
Sometimes the results confirm that the antibiotic already prescribed is appropriate. At other times they suggest that a different antibiotic may work better.
Why should I provide a sputum sample before starting antibiotics?
Whenever possible, it is usually best to collect a sputum sample before starting antibiotics.
Once antibiotics have begun to kill bacteria, it can become more difficult for the laboratory to identify exactly which organisms were present.
This does not mean a sample taken later has no value, but early samples often provide the clearest picture.
What if no bacteria are found?
A negative culture does not always mean that nothing is wrong.
There are several possible reasons. The infection may have been caused by a virus, you may already have started antibiotics, the bacteria may be difficult to grow in the laboratory, or your symptoms may be due to worsening aspergillosis or inflammation rather than a bacterial infection.
Your doctor will interpret the laboratory results alongside your symptoms, examination and any imaging studies.
Can my sputum change over time?
Yes. The bacteria living in the lungs can change over months or years. Some may disappear, while others become more common. Occasionally bacteria develop resistance to antibiotics that previously worked well.
For this reason, previous sputum results remain useful, but they do not always predict what is causing your current infection.
Did you know?
A sputum sample does more than identify bacteria. It can also help your healthcare team avoid unnecessary antibiotics, detect resistant organisms, monitor long-term changes and, in some patients, identify fungi or other less common causes of infection.
The future of laboratory testing
Traditional cultures remain extremely important, but laboratory diagnosis is continuing to evolve.
Researchers are developing faster molecular tests that may identify bacteria, fungi and antibiotic resistance genes within hours rather than days. These new technologies are expected to play an increasingly important role in helping doctors prescribe the right antibiotic as quickly as possible.
7. Why don’t doctors always prescribe antibiotics?
Many people expect antibiotics whenever a chest condition worsens. If you have previously benefited from antibiotics, it can be frustrating when a doctor decides that they are not needed this time.
However, not every increase in cough, sputum or breathlessness is caused by a bacterial infection. Prescribing antibiotics when they are unlikely to help exposes you to possible side effects without treating the underlying problem.
Not every flare-up is a bacterial infection
Many different problems can produce similar symptoms.
Increased cough, tiredness or breathlessness may be caused by a bacterial chest infection, a viral infection such as influenza or COVID-19, a flare-up of aspergillosis, increased airway inflammation, poor mucus clearance, an asthma or COPD exacerbation, heart problems or another medical condition.
Key message
Antibiotics only work against bacteria. If your symptoms are caused by something else, an antibiotic is unlikely to help and may expose you to unnecessary risks.
Doctors weigh up the benefits and risks
Every prescription involves balancing potential benefits against possible harms.
Before recommending an antibiotic, your healthcare professional will consider how likely a bacterial infection is, how unwell you are, whether waiting for further information is safe, whether another condition could explain the symptoms, what side effects or drug interactions might occur, and whether you have received several recent courses of antibiotics.
Sometimes the safest decision is to monitor symptoms closely, arrange investigations or review you again rather than prescribing antibiotics immediately.
Antibiotics are not risk-free
Although antibiotics save countless lives, they can also cause unwanted effects.
Depending on the medicine, these may include stomach upset or diarrhoea, allergic reactions, photosensitivity, interactions with other medicines, disturbance of the normal gut microbiome, and encouraging antibiotic-resistant bacteria.
What is a delayed prescription?
Occasionally your doctor may recommend a delayed or “back-up” antibiotic prescription.
This means you are asked to wait for a short period before starting treatment, or only begin the antibiotic if your symptoms worsen or fail to improve.
Delayed prescribing can reduce unnecessary antibiotic use while still ensuring treatment is available if it becomes needed. It is not appropriate for every patient or every infection, but it is one of several approaches doctors may use.
People with chronic lung disease may need a different approach
For people with bronchiectasis or aspergillosis, treatment decisions are often more individual than they are for otherwise healthy adults.
Your respiratory specialist may recommend that you provide a sputum sample at the start of a flare-up, contact your specialist team promptly, keep “rescue antibiotics” at home if this forms part of your agreed care plan, or attend hospital if your symptoms are severe.
Always follow the management plan agreed with your healthcare team, as this will take account of your own medical history and previous infections.
Remember
Choosing not to prescribe antibiotics is an active medical decision, not simply the absence of treatment. Your healthcare professional may recommend monitoring, investigations or a different treatment because they believe this is the safest and most appropriate approach.
Knowing when to seek urgent medical advice
Although not every flare-up requires antibiotics, some symptoms should never be ignored.
Seek urgent medical advice if you develop significant or increasing breathlessness, persistent high fever or rigors, confusion or increasing drowsiness, new chest pain, large amounts of blood when coughing, or rapidly worsening symptoms.
If you are unsure, contact your healthcare team or seek urgent medical assessment.
8. Side effects: what should I watch for?
Like all medicines, antibiotics can cause side effects. Fortunately, most people complete a course without experiencing any serious problems. Many side effects are mild, temporary and disappear once treatment has finished.
However, every antibiotic has its own pattern of possible side effects, which is one reason your healthcare professional carefully considers which medicine is most appropriate for you.
Key message
Most side effects are mild and manageable, but it is important to know which symptoms are expected, which should be reported to your healthcare team, and which require urgent medical attention.
Common side effects
The most frequently reported side effects include nausea, stomach discomfort, diarrhoea, loss of appetite, metallic or altered taste, and thrush affecting the mouth or vagina.
These symptoms are usually temporary and improve after the antibiotic has been completed.
Photosensitivity: when sunlight becomes a problem
Some antibiotics, including doxycycline, can make your skin much more sensitive to sunlight and ultraviolet light. This is known as photosensitivity.
People affected may develop severe sunburn much more quickly than usual, even after relatively short periods outdoors.
This is not only relevant on holiday or during hot weather. Some people may burn more easily while gardening, walking the dog, sitting near strong sunlight, driving, or spending time outdoors on a bright day.
While taking medicines that cause photosensitivity it is sensible to avoid prolonged exposure to strong sunlight, wear protective clothing and a wide-brimmed hat if outdoors, use a broad-spectrum sunscreen with a high SPF, and avoid sunbeds.
If you develop an unusually severe skin reaction after sun exposure, contact your healthcare professional.
Allergic reactions
Some people are allergic to particular antibiotics, especially those in the penicillin family.
Symptoms may include a widespread itchy rash, swelling of the lips, tongue or face, difficulty breathing, wheezing, collapse or feeling faint.
Severe allergic reactions, also known as anaphylaxis, are medical emergencies and require immediate emergency treatment.
Looking after your gut
Antibiotics do not distinguish between harmful bacteria causing an infection and many of the helpful bacteria that naturally live in the gut.
As a result, some people develop diarrhoea or other digestive symptoms during treatment.
Most people recover naturally after finishing their antibiotics as their normal gut bacteria gradually re-establish themselves.
Other important side effects
Although less common, some antibiotics have specific side effects that your healthcare professional may discuss with you.
Examples include tendon inflammation or rupture with some fluoroquinolone antibiotics, hearing or balance problems with certain intravenous antibiotics, effects on kidney function, effects on liver function, and changes in heart rhythm with some medicines.
These problems are uncommon, but they illustrate why different antibiotics are chosen carefully for different patients.
Why does my doctor ask about previous side effects?
If you have experienced troublesome side effects before, it is important to tell your healthcare professional.
For example, if you previously developed severe diarrhoea, a significant skin reaction or marked photosensitivity while taking a particular antibiotic, your doctor may choose a different treatment if a suitable alternative is available.
Keeping a personal record of important side effects can be extremely helpful, particularly if you receive care from several different healthcare providers.
When should I seek medical advice?
Contact your healthcare team promptly if you develop persistent or severe diarrhoea, a widespread rash, yellowing of the skin or eyes, new hearing problems, severe dizziness, pain or swelling in a tendon, or any side effect that concerns you.
Seek emergency medical help immediately if you develop swelling of the face or throat, severe difficulty breathing or symptoms of anaphylaxis.
9. Drug interactions: why does my doctor need to know about every medicine I take?
People living with aspergillosis often take several medicines at the same time. These may include antifungal medicines, inhalers, corticosteroids, treatments for asthma or bronchiectasis, blood pressure tablets, blood thinners and medicines for other long-term conditions.
When a new antibiotic is prescribed, your healthcare professional will usually check whether it could interact with any of your existing medicines.
Most interactions can be avoided simply by choosing a different antibiotic or by monitoring treatment more closely.
Key message
Always tell your doctor, nurse or pharmacist about every medicine you take, including inhalers, over-the-counter medicines, vitamins, herbal remedies and dietary supplements.
What is a drug interaction?
A drug interaction occurs when one medicine changes the way another medicine works.
An interaction may make one medicine less effective, increase the chance of side effects, increase or decrease the amount of a medicine in the bloodstream, or require additional monitoring during treatment.
Not every combination causes problems, but checking for interactions is an important part of safe prescribing.
Why is this particularly important in aspergillosis?
Many people with aspergillosis receive antifungal medicines such as itraconazole, voriconazole, posaconazole or isavuconazole.
These medicines can be highly effective, but they are also well known for interacting with a wide range of other drugs.
Before prescribing an antibiotic, your healthcare professional may therefore review your current medicines to make sure the combination is appropriate.
Other medicines that may interact
Depending on the antibiotic being prescribed, your healthcare professional may also consider interactions with corticosteroids, blood-thinning medicines, heart rhythm medicines, diabetes treatments, anti-epileptic medicines, some cholesterol-lowering medicines, certain antidepressants and biological therapies used for severe asthma.
This does not mean these medicines cannot be used together. In many cases they can, but careful selection and monitoring are important.
Timing can also matter
Some medicines can reduce how well an antibiotic is absorbed.
For example, certain antibiotics should not be taken at exactly the same time as calcium supplements, iron tablets, magnesium-containing indigestion remedies or zinc supplements.
Your pharmacist or healthcare professional will advise you if medicines need to be separated by a few hours.
Don’t forget non-prescription medicines
Many people assume that only prescription medicines matter.
However, over-the-counter medicines, herbal preparations and food supplements can also interact with prescription medicines.
Always mention anything you are taking, even if you bought it yourself or only use it occasionally.
Did you know?
Community pharmacists routinely check for many potential drug interactions before dispensing medicines. They are an excellent source of advice if you are unsure whether medicines can safely be taken together.
Keeping an accurate medicines list
If you have a chronic lung condition, one of the most useful things you can do is keep an up-to-date medicines list.
This should include prescription medicines, inhalers, antifungal medicines, regular antibiotics, rescue medicines, vitamins and supplements, and any known drug allergies or important side effects.
Having this information available can be particularly helpful if you are admitted to hospital, attend an emergency department or see a healthcare professional who is unfamiliar with your medical history.
Further information
Aspergillosis.org has detailed guides covering antifungal medicines and their interactions. If you take an antifungal medicine, these resources provide more detailed information about specific drug combinations and precautions.
10. Antibiotics and the microbiome
Over the past decade, scientists have become increasingly interested in the microbiome: the enormous community of bacteria, fungi and other microorganisms that naturally live in and on our bodies.
Most of these organisms are harmless and many play an important role in maintaining health. They help digest food, produce vitamins, support the immune system and compete with potentially harmful microbes.
Antibiotics are designed to kill disease-causing bacteria, but they can also affect many helpful bacteria at the same time.
Key message
Antibiotics save lives and remain one of the greatest advances in modern medicine. However, researchers are learning that they may also temporarily alter the body’s normal microbiome. Understanding these changes is helping doctors use antibiotics more wisely.
What is the microbiome?
Your body is home to trillions of microorganisms. These communities are found in many places, including the gut, mouth, skin, nose and lungs.
Together they form your microbiome. Although invisible, these microorganisms are an important part of normal human biology.
How do antibiotics affect the microbiome?
Because antibiotics cannot always distinguish between harmful and helpful bacteria, they may reduce the numbers of beneficial bacteria as well as those causing an infection.
This helps explain why some people experience diarrhoea, changes in bowel habit, thrush or digestive discomfort during or shortly after antibiotic treatment.
For most people, the microbiome gradually recovers after treatment has finished, although recovery may take time and varies between individuals.
Why are researchers so interested?
Scientists are now investigating whether the microbiome influences many aspects of health, including immunity, inflammation and susceptibility to infection.
This is an exciting area of research, but many questions remain unanswered.
Researchers are still working to understand which changes are temporary, which are important for long-term health, how repeated antibiotic courses affect the microbiome, and whether it is possible to protect beneficial bacteria while still treating infection effectively.
The microbiome has become an area of intense research, but scientists are still learning which changes are important and how they influence long-term health.
What about people with chronic lung disease?
People living with bronchiectasis and aspergillosis may receive repeated courses of antibiotics over many years.
Researchers are therefore particularly interested in understanding how long-term antibiotic treatment influences both the gut microbiome and the community of microorganisms living within the airways, sometimes called the lung microbiome.
This research may help explain why some people experience repeated infections while others remain relatively stable, although many questions have yet to be answered.
Should I take probiotics?
This is one of the questions patients ask most often.
Some studies suggest that certain probiotics may reduce the risk of antibiotic-associated diarrhoea in some people. However, not every probiotic is the same, and research is continuing to determine which products are beneficial, who is most likely to benefit, and when they should be used.
For most people, eating a balanced diet that supports general health is more important than taking a particular probiotic supplement.
If you have a weakened immune system or are receiving specialist treatment, speak to your healthcare team before taking probiotic products, as they may not be suitable for everyone.
Be cautious of marketing claims
Many products are marketed as “microbiome boosters”, “gut health” supplements or “immune support” products. Some may be harmless, but the quality of evidence varies. Be especially cautious about products that claim to prevent infection, replace medical treatment or “repair” the microbiome quickly.
The future
As our understanding of the microbiome grows, it is likely to influence how antibiotics are developed and prescribed.
Future treatments may become increasingly personalised, helping doctors choose therapies that not only treat infection effectively but also preserve the beneficial microorganisms that contribute to long-term health.
11. Antibiotic resistance: why does it matter?
Antibiotic resistance has become one of the greatest challenges facing modern medicine. Around the world, doctors are seeing increasing numbers of bacteria that have become difficult, or sometimes impossible, to treat using antibiotics that once worked well.
This does not mean antibiotics are no longer effective. Most bacterial infections can still be treated successfully. However, preserving these medicines for the future requires careful use by healthcare professionals, patients, researchers and governments alike.
Key message
People do not become resistant to antibiotics. Bacteria do. Antibiotic resistance develops when bacteria change over time, making some antibiotics less effective against them.
How does antibiotic resistance develop?
Bacteria multiply very quickly.
Occasionally, random genetic changes occur that help some bacteria survive exposure to a particular antibiotic. When antibiotics are used, these resistant bacteria may survive while more susceptible bacteria are killed.
The resistant bacteria can then continue to multiply and, in some cases, spread to other people.
This is a natural process driven by evolution, but the more antibiotics are used, the greater the opportunity for resistant bacteria to be selected.
Why does this matter to me?
If you have a chronic lung condition, antibiotics may be an important part of your treatment throughout your life.
Preserving effective antibiotics is therefore not just a global issue. It is also a personal one.
If bacteria become resistant to commonly used antibiotics, treatment options may become more limited, and future infections may be more difficult to manage.
What is antimicrobial stewardship?
You may hear healthcare professionals talk about antimicrobial stewardship.
This means using antibiotics, antifungals and other antimicrobial medicines carefully and responsibly so that they remain effective for as long as possible.
Antimicrobial stewardship is about giving every patient the treatment they need, not denying treatment to reduce costs.
Good antimicrobial stewardship aims to treat infections promptly and effectively, avoid antibiotics when they are unlikely to help, choose the most appropriate antibiotic, use the correct dose and duration, change to a more targeted antibiotic when laboratory results become available, and reduce the development of antibiotic resistance.
Did you know?
Many hospitals have specialist antimicrobial stewardship teams made up of doctors, pharmacists, microbiologists and infection specialists who work together to ensure antibiotics are used as safely and effectively as possible.
Can patients help?
Absolutely.
You can support good antibiotic stewardship by taking antibiotics exactly as prescribed, providing sputum samples before starting treatment whenever possible, not sharing antibiotics with other people, not keeping leftover antibiotics for future illnesses unless specifically advised as part of your agreed care plan, telling your healthcare team if treatment is not working or if you develop side effects, and keeping an accurate record of previous infections and treatments.
These simple steps help your healthcare team make the best possible treatment decisions.
Are new antibiotics being developed?
Yes, but developing new antibiotics is difficult, expensive and time-consuming.
Unlike many other medicines, antibiotics are usually taken for only a short period, making them less commercially attractive to develop. At the same time, bacteria continually evolve, meaning new medicines may eventually encounter resistance as well.
This is one reason why preserving the antibiotics we already have remains so important.
Resistance is only part of the solution
Modern medicine is increasingly looking beyond simply developing stronger antibiotics.
Researchers are also working on faster diagnostic tests, rapid identification of resistance genes, vaccines that prevent bacterial infections, new ways of targeting bacteria more precisely, and treatments that reduce the need for antibiotics altogether.
The goal is not only to develop new medicines but also to ensure that every patient receives the right antibiotic, at the right time, for the right infection.
12. The future of treating infections
Antibiotics have transformed medicine over the past 80 years, saving millions of lives and making many modern medical treatments possible. Although antibiotic resistance presents a significant challenge, there are many reasons to be optimistic about the future.
Researchers around the world are developing new antibiotics, faster diagnostic tests and entirely new ways of preventing and treating infections. The aim is not simply to find “stronger” antibiotics, but to ensure that every patient receives the right treatment at the right time.
Key message
The future of infection treatment is becoming more precise, personalised and evidence-based. Better diagnostics may be just as important as new antibiotics in improving patient care.
Faster diagnosis
One of the biggest changes is likely to be how quickly infections can be identified.
Traditional laboratory cultures remain extremely important, but they can take several days to provide complete results.
New molecular techniques, including PCR and genetic sequencing, are increasingly able to identify bacteria, fungi and important resistance genes much more quickly. In the future, doctors may be able to select the most appropriate treatment within hours rather than days.
This is particularly exciting for people with chronic lung disease, where identifying the cause of an infection quickly may help avoid unnecessary antibiotics and improve outcomes.
New antibiotics
Although developing new antibiotics is scientifically challenging, research continues around the world.
Many newer antibiotics are being designed to treat bacteria that have become resistant to older medicines, particularly those responsible for serious hospital-acquired infections.
However, researchers recognise that simply developing new antibiotics is not enough. Every new antibiotic must also be protected through careful prescribing so that it remains effective for as long as possible.
Precision medicine
Instead of treating every patient in the same way, doctors increasingly aim to tailor treatment to the individual.
Future decisions may take account of the exact bacteria causing the infection, their resistance profile, your previous microbiology results, your underlying lung disease, your medicines and possible drug interactions, and even your own microbiome.
This personalised approach aims to improve treatment while reducing unnecessary antibiotic exposure.
Artificial intelligence
Artificial intelligence may assist researchers and healthcare professionals in several areas of infection management.
Potential future applications include interpreting laboratory results more rapidly, predicting antibiotic resistance, helping clinicians select the most appropriate treatment, and identifying patients at greatest risk of severe infection.
AI is expected to support, not replace, the judgement of experienced healthcare professionals.
Bacteriophage therapy
One of the most fascinating areas of research involves bacteriophages, often shortened to phages.
These are naturally occurring viruses that infect bacteria rather than people.
Scientists are investigating whether carefully selected phages could be used to treat some infections that no longer respond well to conventional antibiotics. Although phage therapy is not yet routine clinical practice, it offers exciting possibilities for the future.
Vaccines and prevention
Perhaps the best way to reduce antibiotic use is to prevent infections from occurring in the first place.
Vaccination programmes, improved infection prevention, better management of chronic lung disease and healthier lifestyles all contribute to reducing the need for antibiotics.
For people living with aspergillosis, measures such as airway clearance, prompt investigation of new symptoms and regular follow-up with their healthcare team may also help reduce the impact of recurrent infections.
Protecting the microbiome
Researchers are also exploring ways of treating infections while causing less disruption to the body’s normal bacteria.
Future antibiotics may become much more selective, targeting harmful bacteria while preserving beneficial microorganisms that support normal health.
This could reduce side effects and help maintain a healthier microbiome during treatment.
Looking to the future
Although headlines often focus on antibiotic resistance, the wider picture is encouraging. Advances in diagnostics, genomics, microbiology, infection prevention and new antimicrobial therapies are changing the way infections are managed. For people living with aspergillosis and bronchiectasis, these developments offer real hope that future treatment will become faster, more targeted and increasingly personalised.
13. Five practical things patients can do
Understanding antibiotics does not mean choosing treatment for yourself. It means being better prepared to work with your healthcare team.
- Provide sputum samples early when your healthcare team asks for them, ideally before starting antibiotics if this is safe and practical.
- Keep a record of previous antibiotics, sputum results, side effects and which treatments seemed to help.
- Tell your doctor and pharmacist about all medicines, including antifungals, inhalers, over-the-counter medicines and supplements.
- Take antibiotics exactly as prescribed and ask for advice if you are unsure what to do.
- Seek medical advice promptly if symptoms worsen, side effects are severe, or you develop warning signs such as increasing breathlessness, chest pain, confusion or coughing up significant amounts of blood.
A final thought
Antibiotics remain one of the greatest achievements in modern medicine. They have saved countless lives and continue to play a vital role in treating bacterial infections.
For people living with aspergillosis and bronchiectasis, antibiotics may be an important part of care, but they need to be used thoughtfully. The best antibiotic is not always the broadest or newest medicine. It is the one that is most likely to treat the infection safely, effectively and with the least unnecessary harm.
Understanding how antibiotics are chosen, why they are used carefully and how research is shaping the future can help patients become informed partners in their own care. By working together, patients and healthcare professionals can help ensure that these remarkable medicines remain effective for future generations.
Internal Links
Consider linking to:
- Antifungal medicines
- Bronchiectasis Knowledge Hub
- Sputum sampling
- Understanding sputum cultures
- Antimicrobial stewardship
- Drug interactions
- Photosensitivity with antibiotics
- Living with bronchiectasis
- Pseudomonas infections
- When to seek urgent medical advice
External References
Useful authoritative resources include:
- NHS guidance on antibiotics
- UK Health Security Agency information on antimicrobial resistance
- National Institute for Health and Care Excellence antimicrobial prescribing guidance
- World Health Organization resources on antimicrobial resistance