General interest

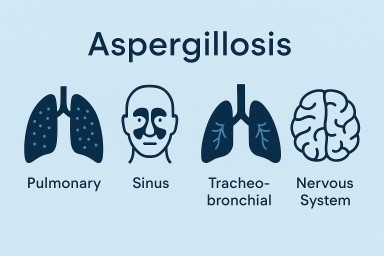
🫁 Mucus Plugging in Aspergillosis: What It Is, Why It Happens, and What It Means
For patients with ABPA, CPA,…


🌫️ A Life Shaped by Mould: One Person’s Journey with CPA and Lung Disease
Sadly, at the time of writing…
For patients with ABPA, CPA,…
Sadly, at the time of writing…