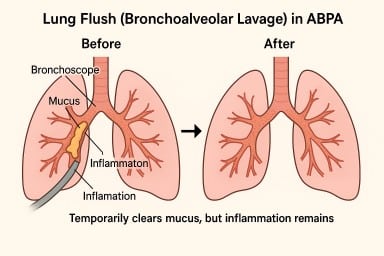
🫁 “Lung Flush” (Bronchoalveolar Lavage) in ABPA – What It Is and Why It Brings Only Short-Term Relief
A lung flush (also called a bronchoalveolar lavage, or BAL) isn’t a regular treatment for Allergic Bronchopulmonary Aspergillosis (ABPA), but it’s sometimes used selectively in NHS hospitals.
💧 What Happens During a Lung Flush
It’s done during a bronchoscopy, where a thin, flexible tube is passed through the nose or mouth into the lungs.
A small amount of sterile saline is washed into part of the lung and then gently suctioned back out.
The fluid is tested for:
-
Aspergillus growth or DNA
-
Other infections (bacteria, fungi, viruses)
-
Signs of inflammation or allergic activity
You’re given local anaesthetic and light sedation, so you stay comfortable but sleepy. Most people go home the same day.
🧪 Main Purpose – Diagnosis
In most ABPA cases, a lavage is done to find out what’s causing symptoms – whether they’re due to Aspergillus, another infection, or ongoing inflammation.
The results help doctors fine-tune treatment, such as adjusting antifungal doses or deciding if a biologic drug might help.
🫁 Sometimes Used to Clear Mucus
In certain situations – especially when thick mucus plugs are blocking airways or causing part of a lung to collapse – doctors may use lavage as a therapeutic “flush.”
This can wash out sticky secretions and temporarily improve airflow, helping physiotherapy and medication work more effectively.
It’s usually a short, day-case procedure, and most people feel back to normal after a day or two.
⚠️ Why It’s Only Short-Term Relief
Although lavage can clear mucus, ABPA is caused by an allergic immune reaction, not by the mucus itself.
Unless that reaction is controlled with:
-
Corticosteroids (to reduce inflammation),
-
Antifungal drugs (to lower the fungal load), or
-
Biologic injections (to block allergy pathways),
…the lungs will continue to produce thick, sticky mucus, which can re-accumulate within days or weeks.
So while a “lung flush” can make breathing easier in the short term, the effect is temporary – like clearing a blocked drain while the tap is still running.
⚠️ Risks and After-Effects
A bronchoscopy with lavage is generally safe, but it is still an invasive procedure. Possible effects include:
-
Temporary sore throat, cough, or hoarseness (common)
-
Mild bleeding or streaks of blood in sputum for a short time
-
Low oxygen levels during or after the procedure (monitored carefully)
-
Chest tightness, infection, or fever – uncommon but possible
-
Bronchospasm (airway narrowing) in people with very sensitive lungs, which is why it’s done in a hospital with respiratory support available
Because of these small but real risks, the NHS uses lavage only when the benefits outweigh the downsides – for example, when mucus is causing serious blockage or when test results will change management.
💬 In Summary
A “lung flush” can temporarily clear mucus and ease breathing, but it doesn’t stop ABPA’s underlying allergic inflammation.
The mucus often returns unless that inflammation is brought under control with long-term medical treatment.
It’s a useful tool when needed, but not something done regularly or lightly.
🌟 Vitamin B12 (Cobalamin) and Iron – What Patients Should Know
People living with chronic lung or fungal conditions sometimes develop low vitamin B12 or iron, especially if appetite, diet, or absorption are affected.
Here’s how to understand your results and treatment options.
🌟 Vitamin B12 (Cobalamin)
✅ What’s a Normal B12 Level?
| Level (pmol/L) | What It Means |
|---|---|
| > 300 | Normal |
| 200–300 | Borderline – may need extra tests (e.g. MMA or homocysteine) |
| < 200 | Deficiency likely |
Some labs report B12 in ng/L — the ranges are similar. Your doctor will interpret them based on the lab reference range.
⚠️ What Happens If B12 Is Low?
Low B12 can cause:
-
Fatigue and weakness
-
Brain fog or memory issues
-
Numbness or tingling in hands or feet
-
Low mood or irritability
-
In severe cases, nerve damage
💉 B12 Treatment
| Cause | Typical Treatment |
|---|---|
| Dietary deficiency (e.g. vegan diet) | High-dose oral B12 tablets or injections |
| Pernicious anaemia (autoimmune) | Lifelong B12 injections every 8–12 weeks |
| Malabsorption (gut issues) | Long-term injections often required |
In the UK, injections are usually hydroxocobalamin 1 mg every 2–3 months for maintenance, after an initial “loading phase” (several doses over 2 weeks).
🌟 Iron (Ferritin and Haemoglobin)
✅ Key Iron Markers
| Test | Normal Range (Women) | What Low Levels Mean |
|---|---|---|
| Ferritin | 30–200 µg/L (some doctors prefer >50) | Reflects iron stores — low = iron deficiency |
| Haemoglobin | 120–160 g/L | Measures oxygen-carrying capacity — low = anaemia |
You can have low iron without anaemia (low ferritin, normal Hb) or both together.
💉 Iron Infusions (e.g. Ferinject)
Used when:
-
Iron tablets don’t work or cause side effects
-
Iron levels are very low or symptoms severe
-
Ongoing blood or iron loss (e.g. heavy periods, inflammatory bowel disease)
Iron infusions raise levels more quickly than tablets. Some people need repeat infusions every 6–12 months depending on the cause.
🔄 Ongoing Monitoring and Follow-Up
| Condition | Typical Follow-Up |
|---|---|
| Low B12 (pernicious anaemia) | Injections for life; blood tests yearly |
| Low B12 (diet-related) | May stop if diet improves and levels remain stable |
| Iron deficiency (no bleeding cause) | Tablets for 3–6 months, then reassess |
| Chronic iron loss (e.g. periods, IBD) | Maintenance iron or repeat infusions |
✅ Reliable Information Sources
📣 Final Advice
If you’re unsure about your test results or treatment:
-
Ask your GP for a copy of your blood test results
-
Request a referral to a dietitian or haematologist
-
Agree a treatment plan and review dates
Always let your healthcare team know if you’re feeling more tired, dizzy, or unwell — sometimes simple tests and supplements make a big difference.

Share your feedback about your care at the National Aspergillosis Centre
There’s now a new way to read and share patient feedback about local NHS hospitals online. All comments come directly from patients and carers.
That’s because NAC sits within the Infectious Diseases service, which is managed through North Manchester as part of the new Manchester University NHS Foundation Trust (MFT) structure.

💬 Healthwatch: Your Local Voice in the NHS
Living with a long-term lung condition such as aspergillosis, asthma, or bronchiectasis often means regular contact with hospitals, GPs, and community clinics.
Sometimes things work well — and sometimes they don’t.
That’s where Healthwatch comes in.
Healthwatch is an independent organisation that represents patients and the public.
It exists to make sure your experiences help shape the way NHS and social-care services are delivered.
🏛️ What is Healthwatch?
Healthwatch was set up by law to be the official voice of patients and the public in health and social care.
There are two levels:
-
Healthwatch England – works nationally to influence NHS and government policy
-
Local Healthwatch – works in every local authority area across England, gathering feedback from people using local services
Healthwatch is not part of the NHS, and it’s not a complaints service, but it does have statutory powers to:
-
Listen to people’s experiences of care
-
Report issues and make recommendations to the NHS, local councils, and care providers
-
Request responses from organisations it investigates
-
Escalate serious concerns to the Care Quality Commission (CQC)
Learn more on the Healthwatch website.
🌿 Why Healthwatch matters to aspergillosis patients
People living with chronic lung disease often face delays, limited understanding, or difficulties accessing ongoing support.
Healthwatch helps make sure those experiences aren’t ignored.
1. Raising the patient voice
You can share your experience of healthcare — good or bad — with your local Healthwatch.
They collect stories from across the community and use them to:
-
Identify patterns (for example, problems with accessing respiratory clinics or antifungal monitoring)
-
Produce reports and recommendations for local NHS decision-makers
-
Push for improvements to long-term care pathways and community support
2. Helping to improve new neighbourhood health hubs
As NHS care moves into the community, Healthwatch plays a key role in making sure new Neighbourhood Health Hubs are:
-
Accessible for people with limited mobility or oxygen needs
-
Located where public transport and parking work for patients
-
Designed with chronic-illness patients in mind, not just short-term care
You can feed in your ideas through Healthwatch about what’s working and what isn’t in new NHS community models.
3. Providing information and signposting
If you’re unsure where to go for care — GP, hospital, or new health hub — or how to complain or appeal a service decision, Healthwatch can point you in the right direction.
They offer clear, local information about:
-
NHS patient transport
-
The Healthcare Travel Costs Scheme (HTCS)
-
Local support groups and community services
4. Supporting patient involvement
Healthwatch works with NHS organisations to include patients and carers in planning and reviewing services.
If you’d like to get involved as a patient representative or share your experience of aspergillosis services, Healthwatch can help you join local working groups or consultations.
5. Spotlighting inequalities
Healthwatch highlights where certain groups are left behind — for example:
-
People with rare or complex conditions
-
Patients in rural or deprived areas
-
Those unable to use digital appointment systems
This helps ensure people with chronic lung conditions are not overlooked when new community-care models are designed.
⚖️ What Healthwatch can — and can’t — do
| ✅ Healthwatch can | 🚫 Healthwatch can’t |
|---|---|
| Collect and report your experience to NHS leaders | Fix individual clinical problems directly |
| Influence NHS and council decisions | Guarantee faster treatment or appointments |
| Provide advice on local services and support | Replace legal or complaints services |
| Escalate major safety concerns to the CQC | Act as your personal advocate in disputes |
Even so, their influence can be powerful — many improvements in NHS access and transport have started with patient stories collected by Healthwatch.
📍 How to contact your local Healthwatch
Every local area has its own Healthwatch website and phone number.
You can find yours at:
👉 Find your local Healthwatch
When you contact them, you can:
-
Fill in a short online form to share your story
-
Ask to join a focus group or consultation
-
Request accessible information or help finding services
-
Subscribe to local updates and reports
If you’d like support from the aspergillosis community, NAC CARES can also help you write or submit your feedback.
💬 Why this matters
“Nothing about us without us.”
Healthwatch exists so that patients — including those with rare and chronic conditions like aspergillosis — can make their experiences count.
By telling your story and feeding back to Healthwatch, you help shape better care for yourself and for others who will face similar challenges in future.

🏥 NHS Neighbourhood Health Hubs: How Community Care Will Work for People with Aspergillosis and Asthma
The NHS is changing how healthcare is delivered — with more care moving closer to home and fewer hospital visits.
A new model called Neighbourhood Health Services (or Neighbourhood Health Hubs) is being rolled out across England from late 2025, and it could make a real difference for people living with aspergillosis, asthma, bronchiectasis, and other long-term respiratory conditions.
🌍 Why care is moving into the community
The goal is to:
-
Bring care to where people live, not just in large hospitals
-
Reduce waiting times by shifting routine tests and reviews out of hospital clinics
-
Join up GPs, nurses, pharmacists, and hospital specialists into one local team
-
Focus on prevention, self-management, and early support
These reforms come from the government’s Healthcare on Your Doorstep announcement (September 2025), supported initially by £10 million across 43 pilot areas in England.
🧑⚕️ What a “Neighbourhood Health Hub” looks like
A one-stop local health centre bringing together:
-
GPs and practice nurses
-
Respiratory nurses, physiotherapists, and pharmacists
-
Mental-health and wellbeing workers
-
Dietitians, occupational therapists, and social-prescribing link staff
-
Voluntary and community organisations (e.g. NAC CARES, Asthma + Lung UK)
Some hubs will connect directly to Community Diagnostic Centres (CDCs) – local sites providing CT, MRI, X-ray, lung-function and blood tests through the NHS England diagnostics programme.
The aim is for one joined-up team to share your records and plan your care locally.
🩺 How hubs work with your GP and A&E
The new hubs are designed to fill the gap between GP surgeries and hospitals – giving extra support when you’re too unwell to manage alone but don’t need emergency care.
🏠 Your GP surgery
You’ll stay registered with your usual GP. They remain in charge of your prescriptions, results, and overall care.
Your GP can now refer you to a Neighbourhood Health Hub for things that need a wider team – for example:
-
Antifungal monitoring or blood tests
-
Lung-function or CT scans
-
Flare-up review by respiratory nurses
-
Fatigue or wellbeing support
🧑⚕️ The Neighbourhood Health Hub
You might go here instead of hospital for:
-
Same-day assessment of an infection or flare-up
-
Bloods, ECGs, or scans ordered by your GP
-
Physiotherapy, airway-clearance or rehabilitation
-
Medication reviews with a pharmacist
-
Appointments with dietitians or mental-health staff
-
Practical help from link workers (see below)
🚨 A&E (Emergency Department)
Still essential for serious problems such as:
-
Sudden or severe breathlessness not relieved by treatment
-
Coughing up blood
-
Chest pain, fainting, or collapse
-
High fever with confusion
If unsure, call NHS 111 or 999 in an emergency.
🔁 When to use which service
| Situation | Who decides | Where you’ll be seen |
|---|---|---|
| Routine check-up or repeat prescription | You / GP | GP surgery |
| Specialist review or complex medication | GP / consultant | Neighbourhood Hub |
| Mild flare-up needing same-day care | NHS 111 / GP | Hub or GP |
| Emergency or life-threatening symptoms | NHS 111 / 999 | A&E / hospital |
| Diagnostic tests | GP / hospital referral | Community Diagnostic Centre |
All sites will share your digital care record so results and updates reach your GP and hospital team automatically.
🧑🤝🧑 Link workers and care coordinators – local help through your GP
Every GP practice and neighbourhood team now has link workers (also called care coordinators or social prescribers).
They’re there to help you navigate healthcare and community support. They can:
-
Arrange or advise on transport for appointments
-
Help complete travel cost reimbursement or benefit forms
-
Connect you with volunteer driver schemes or local charities
-
Find exercise, wellbeing, or peer-support groups
-
Support with fatigue, isolation, or anxiety
Ask your GP reception or Neighbourhood Hub to refer you to the link worker, or request a call-back via the NHS App.
🚗 Transport and accessibility
🚐 NHS Patient Transport Service (PTS)
If you can’t use public transport for medical reasons (for example, oxygen use, mobility difficulties, or severe fatigue), you may qualify for free NHS transport.
Your GP, link worker, or hospital can book this for you through the regional PTS (for example, NWAS in the North West).
💷 Healthcare Travel Costs Scheme (HTCS)
If you’re on a low income or certain benefits, you can reclaim travel expenses under the HTCS.
Bring your appointment letter and proof of eligibility, or ask your link worker to help with the form.
🚙 Community & volunteer transport
Each Integrated Care System (ICS) works with local councils and charities such as Age UK, Mind, or Good Neighbour schemes to run community minibuses and volunteer driver services.
Ask your link worker or hub team for local options.
🅿️ Accessibility
All new and refurbished hubs must include:
-
Blue Badge parking and drop-off zones
-
Wheelchair-friendly entrances and toilets
-
Seating and oxygen-safe waiting areas
-
Negotiated free or reduced parking in shared sites
🧭 At a glance
| Issue | What’s planned | What to do now |
|---|---|---|
| Public transport | Sites chosen to be local, but not always central | Check routes before your visit |
| NHS Patient Transport | Still available for medical need | Ask GP or link worker to book |
| Travel-cost reimbursement | Continue via HTCS | Keep proof of benefit |
| Community / volunteer drivers | Expanding under ICB–VCS partnerships | Request info via link worker |
| Disabled parking / drop-off | Required at new sites | Confirm when booking |
🪶 A message from the aspergillosis community
For many people with lung disease, “local care” only works if it’s accessible care.
Groups such as NAC CARES, Asthma + Lung UK, and Healthwatch are urging NHS leaders to:
-
Design transport and parking into every new site
-
Ask about mobility and oxygen needs when booking
-
Fund local volunteer schemes
-
Provide dedicated link workers at every hub and GP practice
If you struggle to reach appointments, tell your clinic or Healthwatch — your feedback shapes how services develop.
🧾 Questions to ask before your first visit
-
🚗 Is there Blue Badge or patient parking on site?
-
🚌 What public-transport links serve the hub?
-
🚐 Can the clinic arrange NHS Patient Transport?
-
💷 Can I claim travel costs under the HTCS scheme?
-
♿ Is the building accessible for wheelchairs or oxygen users?
-
💨 Are there rest areas for people who get breathless?
-
🧑🤝🧑 Can my carer or partner attend with me?
-
👩💼 Is there a link worker who can help with transport or forms?
-
🕓 Are there quiet waiting spaces to reduce infection risk?
Having these answers before your appointment makes your visit smoother and safer.
💬 Final thought
“Neighbourhood care” isn’t about replacing your GP or A&E — it’s about bridging the gap.
The new hubs aim to bring together your GP, hospital specialists, and community teams in one local setting, providing earlier help, fewer hospital journeys, and care designed around your life, not your postcode.
🔎 Behind the Headlines: Is this an NHS Expansion or a Shift?
Many people wonder whether this is new investment or a reshuffle of existing NHS services.
🧱 What’s really happening
-
The Neighbourhood Health Service is not a new tier of the NHS, but a redesign of how GP, hospital, and community teams work together.
-
The focus is on moving care out of hospitals and into local clinics, using the same staff and budgets more effectively.
-
Hospitals will still handle emergencies and complex cases, but routine tests, reviews, and education will move into the hubs.
⚖️ Expansion or movement?
| Area | Expansion | Reorganisation |
|---|---|---|
| Buildings | Some new or refurbished hubs and diagnostics centres | Many reusing existing GP or community facilities |
| Staffing | Some new link workers, pharmacists, and AHPs | Most existing NHS staff redeployed across neighbourhoods |
| Funding | £10m pilot investment + diagnostic capital | No major long-term new funding yet announced |
| Patient benefit | Easier access, joined-up records | May reduce hospital appointments rather than add capacity |
💬 What this means
For patients, it should feel like an expansion — more care, closer to home —
but in reality it’s a shift of where and how NHS services are delivered, not a large-scale increase in total NHS resources.
⚠️ Risks and opportunities
| Opportunities | Risks |
|---|---|
| Easier local access | Risk of hospital clinics closing before hubs fully staffed |
| Joined-up records | Depends on IT integration |
| Focus on prevention | May feel like hospital services are being reduced |
| Better continuity | Needs clear accountability (GP vs hub) |
🧩 Summary
The new neighbourhood model is a reorganisation within the NHS, not a separate expansion.
It aims to use existing staff, buildings, and budgets more efficiently — giving patients with chronic conditions like aspergillosis and asthma easier access to care and support in their own communities.
🎢 Life as a Patient

Living with chronic illness is often described as a journey, but that word can feel far too calm. In truth, it’s more like a modern roller coaster — fast, unpredictable, and full of twists that catch you off guard.
There are the high climbs, when medication works, energy returns, and hope builds quietly in your chest. Then there are the sudden drops, when symptoms flare, infections hit, or test results turn against you. But what really defines the experience are the loops and spirals — the disorienting moments that spin you upside down, when you’re not sure which way is forward, or how long it will take to steady yourself again.
Each turn tests your courage, your patience, and your ability to keep holding on. Sometimes you’re screaming inside while smiling on the outside. Other times, you find small moments of stillness even as the track twists beneath you — the deep breath between the storms.
And through it all, you learn:
-
To adapt rather than control.
-
To brace and breathe rather than fight every turn.
-
To appreciate those who stay beside you in the carriage, even when the ride is rough.
The roller coaster of illness is not one anyone chooses to board. But it teaches something profound — that strength isn’t about never being scared; it’s about showing up, again and again, when the world flips upside down.
Living Between What My Body Needs and What the World Expects

Sometimes it feels as if people grow tired of hearing about illness or fatigue. They encourage us to “think positively,” as if mindset alone could repair the body or quiet exhaustion.
But chronic illness doesn’t work like that. It’s a daily negotiation between two inner voices — one saying, “You need to rest,” and the other whispering, “You still have responsibilities.” That constant tug-of-war leaves many of us feeling trapped between what our body needs and what life demands.
Even small things — such as changes in weather, sleep patterns, or stress — can tip the balance. We learn to pace ourselves, to weigh every decision, to ration energy. And still, the world around us often sees only the surface: “You look well.”
The Other Side of Positivity
For those who don’t live with chronic illness, this can be difficult to face. Often, people cling to optimism not because they’re unkind, but because they don’t want to confront the truth — that illness can be long-term, unpredictable, and out of anyone’s control.
Positivity can become a shield: a way of keeping the world steady and reassuring when faced with something that can’t be fixed. Saying “You’ll be fine” or “Stay strong” helps them feel hopeful, even if it leaves us feeling unseen.
Understanding that this comes from discomfort, fear, or helplessness rather than indifference can make those moments a little easier.
Where Real Connection Starts
Real empathy sits somewhere between positivity and honesty — where people can acknowledge pain without losing hope.
Most of the world won’t fully understand chronic fatigue or the mental gymnastics it takes to stay balanced until they experience it themselves. But by sharing what it’s really like, we give others the chance to learn — just as society learns to understand invisible struggles like dyslexia or digital exclusion.
Understanding begins when we listen without needing to fix. Sometimes the greatest kindness is simply to say, “That sounds hard — how are you managing today?”
Aspergillus Saga — July 2024 to June 2025: Searching for the Invisible
In this compelling personal account, a patient describes her year-long journey battling what ultimately was identified as subacute invasive aspergillosis. She walks us through months of worsening symptoms, repeated rounds of antifungals, diagnostic uncertainty, and the pivotal decision to undergo lung surgery. The turning point: removal of a single lesion led to a rapid resolution of systemic infection signs, with follow-up therapy and monitoring guided by her infectious disease team. Her story highlights how, with very little precedent in medical literature, patients and clinicians sometimes must walk together on uncharted ground.
👉 Read the full article here:
“Aspergillus Saga – July 2024 to June 2025: Searching for the Invisible” Beauty for Ashes

🧩 NAC Aspergillosis Research Digest — Focus: Chronic Aspergillosis (October 2025: week 42)
🧬 Focus Review — Chronic Aspergillosis (October 2025)
Here are peer-reviewed papers on chronic aspergillosis published in the last month:
1. Improving Diagnostic Sensitivity Using Species-Specific IgG (Sep 2025)
-
This study investigated better blood tests to diagnose CPA by measuring IgG antibodies not just to Aspergillus fumigatus but also to other common Aspergillus species.
-
They found adding antibodies against non-fumigatus species identified more CPA cases that would have been missed by the standard A. fumigatus test alone.
-
The treatment results were similar regardless of which Aspergillus species was involved.
-
This means broader antibody testing improves diagnosis without changing expected outcomes.
- Read full paper on PubMed
2. Prevalence and Impact of Bacterial Co-infections in CPA (April 2025)
-
This study looked at how often bacterial infections occur alongside CPA and their effect on patients.
-
About 21% of CPA patients had bacterial co-infections.
-
However, having a bacterial co-infection did not significantly change mortality rates compared to those without.
-
This highlights the need to assess for bacteria but suggests it may not worsen long-term outcomes.
- Read full paper on PMC
3. Non-invasive Monitoring Using Serology and HRCT Imaging (June 2025)
-
Researchers combined blood antibody tests and high-resolution chest CT scans to identify active Aspergillus infections in chronic lung disease patients.
-
This method distinguished active infections from colonization without invasive procedures.
-
It supports using combined non-invasive tests to decide who needs further invasive diagnostics or antifungal treatment.
-
This approach helps avoid unnecessary treatments and invasive tests.
- Read full paper on Frontiers
In short: these studies improve how doctors diagnose and monitor CPA — by expanding antibody testing beyond classic targets, recognizing the role but limited impact of bacterial co-infections, and using combined non-invasive testing strategies to guide management safely and effectively.
🌦️ Understanding Corticosteroid Mood Swings
Alison shared something that will resonate with many of us:
“Recognising that prednisone mood swings are very unpredictable is a good reminder as I feel like I am up and down so much of late. Yesterday’s swap to half hydrocortisone and half prednisone probably took a bit of adjusting too. Better day today though — I even got out to pick up my campervan that had been in for service. Felt really good to be driving it again and as the weather improves, I live in hope that I might get to use it this year!” 😊🤔
💭 Why mood can change on corticosteroids
Steroid medicines such as prednisone, prednisolone, and hydrocortisone affect many systems in the body — including brain chemistry.
When levels go up or down (for example when changing dose or type), it’s common to feel:
-
Irritable or anxious one day, low or tired the next
-
More emotional than usual — tears or frustration come quickly
-
Sleep disturbance, vivid dreams, or early waking
-
Short bursts of energy or restlessness, followed by a “crash”
These changes don’t mean you’re “losing control” — they reflect how sensitive the brain is to shifts in cortisol, the hormone steroids replace or supplement.
⚖️ Why switching between steroids can feel bumpy
Prednisone and hydrocortisone are both corticosteroids but have different potencies and timings:
| Steroid | Approx. equivalent dose (anti-inflammatory) | Typical duration of action |
|---|---|---|
| Hydrocortisone | 20 mg ≈ 5 mg prednisolone | Short-acting (6–8 hours) |
| Prednisone/Prednisolone | 5 mg | Longer-acting (12–36 hours) |
When switching or mixing them, the body’s rhythm of cortisol can temporarily feel off — like jet lag for your stress hormones. It often settles after a few days.
🌞 Tips that may help
-
Keep a simple mood or energy diary — it helps you and your clinician see patterns.
-
Take doses at consistent times, usually in the morning, unless advised otherwise.
-
Build in gentle activity or time outdoors — small wins, like Alison’s campervan trip, really lift mood.
-
Avoid caffeine or alcohol spikes if feeling restless or irritable.
-
Tell your clinician if mood swings are severe or prolonged — dose adjustment or slower tapering may help.
💬 In Alison’s words
“Better day today.”
Sometimes that’s the victory — one step, one better day, one bit of normality returning.