Side Effects
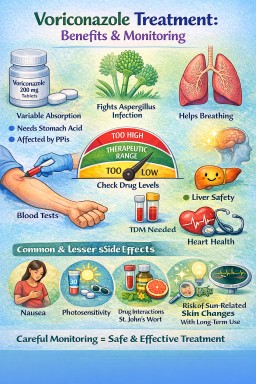
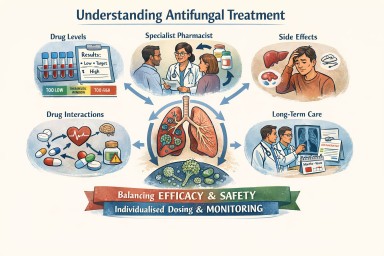


When treatment itself causes harm: an important message for people with aspergillosis
For most people, following…






🌿 Your Immune System, Biologics, and Steroids: What’s Suppressed — and What Stays Strong
A clear, reassuring guide for…
For most people, following…
A clear, reassuring guide for…