Professional Guidance
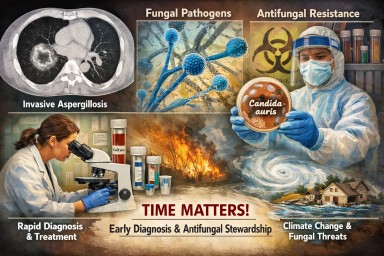
Systemic fungal infections: why speed, diagnosis and stewardship matter
Systemic fungal infections —…


ABPA and Work: What a Patient Poll Tells Us About Employment, Health, and Real-World Impact
An article for patients, GPs,…

Systemic fungal infections —…
An article for patients, GPs,…