Professional Guidance

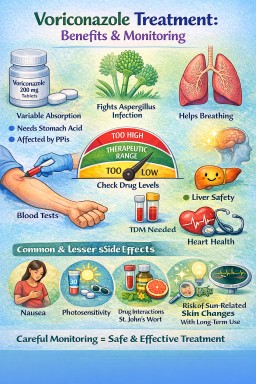
Antifungal drug interactions: what patients with aspergillosis need to know
Last reviewed: April 2026…


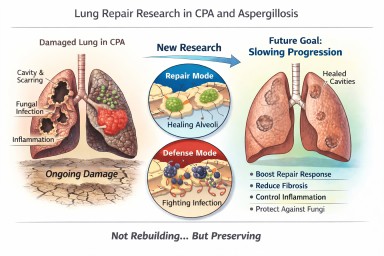
Looking further into the future - could we control lung damage, preserve healthy lung tissue better?
Can Lungs Repair Themselves?…