
Connecting patients, carers, clinicians and scientists to improve life with aspergillosis
World Aspergillosis Day (WAD) is an annual global event that brings together people who live with, care for, treat, and research long-term forms of aspergillosis — particularly chronic pulmonary aspergillosis (CPA) and allergic bronchopulmonary aspergillosis (ABPA).
Each year, WAD creates a shared space where:
-
patients and carers can hear directly from specialists,
-
clinicians and scientists can learn from patient experience,
-
and everyone can explore how new research translates into better care.
🎥 Missed previous events?
Recordings from earlier World Aspergillosis Day meetings are available on our YouTube channel.
📅 NAC World Aspergillosis Day Meeting 2026
The National Aspergillosis Centre (NAC) will once again host a free online meeting:
🗓 Tuesday 3 February 2026
💻 Online via Microsoft Teams
👥 Open to patients, carers, clinicians, scientists, and anyone who lives or works with aspergillosis
🧬 This year’s theme:
“How can the genomics revolution help patients with chronic aspergillosis?”
Why genomics — and why now?
Modern molecular tests such as PCR and DNA sequencing are becoming faster, cheaper and more accurate. Because of this, the NHS is increasingly exploring how genomic technologies can be used to improve diagnosis, monitoring and treatment across many diseases — including aspergillosis.
This year’s WAD meeting will start an open discussion between patients and professionals about which genomic and molecular tests are likely to matter most for people with aspergillosis in the years ahead.
Topics will include:
-
🧠 Is there a “gene for aspergillosis”?
Should people be tested for genetic susceptibility? -
💊 Genes and voriconazole dosing
Can testing the CYP2C19 gene help personalise antifungal treatment? -
🦠 Tracking antifungal resistance
How molecular testing of Aspergillus strains can help hospitals monitor resistance. -
🔬 Aspergillus PCR at NAC
How PCR is already used to diagnose and monitor chronic aspergillosis.
🗣️ Patient voices at the heart of the meeting
As always, patient experience will be central to the day.
This year will include new patient stories, including Alison, who will talk about how her aspergillosis treatment led to the development of adrenal insufficiency, and what that has meant for her care and daily life.
“I don’t know anything about genetics — is this for me?”
Absolutely yes.
You don’t need any background in genetics to take part. Everything will be explained clearly, step by step, with minimal jargon.
Planned discussion topics include:
-
What do my Aspergillus PCR test results actually mean?
-
Is there really a “gene for CPA”?
-
Why do genes matter for antifungal dosing?
In fact, the more questions you ask — especially the “silly” ones — the better. The discussion from the day will be used to create a new patient leaflet, designed to help people better understand their diagnosis and test results.
✅ Registration is now open
🎟 Book your free place via Eventbrite:
👉 www.eventbrite.co.uk/e/world-aspergillosis-day-tickets-1980707139373
💻 Joining via Microsoft Teams
The meeting will be held online using Microsoft Teams, which you can download here:
👉 www.microsoft.com/en-gb/microsoft-teams/group-chat-software
If you haven’t used Teams before, we recommend doing a test call in advance. If you run into any problems setting things up, we’re very happy to help.
We hope you can join us for World Aspergillosis Day 2026 — to learn, to ask questions, and to help shape the future of aspergillosis care together.
Hyper-IgE syndrome
A patient-friendly guide (and why it matters if you have aspergillosis)
It is not the same as having lots of allergies, even though it can look very similar at first.
What is IgE, and why does it matter?
IgE is usually involved in allergies and asthma.
In Hyper-IgE syndrome:
-
IgE levels are extremely high (often many thousands)
-
But the immune system is unbalanced
-
This makes infections—especially in the lungs and skin—harder to control
So IgE is high, but protection is weak.
How might Hyper-IgE syndrome affect everyday life?
Not everyone has the same symptoms, but common features include:
Lung and chest problems
-
Repeated chest infections (often from a young age)
-
Ongoing cough, breathlessness and mucus
-
Lung damage such as bronchiectasis
-
Lung cavities that can later become infected by moulds such as Aspergillus
Skin and infection problems
-
Long-standing eczema or very sensitive skin
-
Recurrent skin infections or boils
-
Infections that keep coming back or take a long time to clear
Other clues (in some people)
-
Frequent infections in childhood
-
Bone or joint problems
-
Dental issues (for example baby teeth not falling out on time)
Why is this important for people with aspergillosis?
For many people, Aspergillus causes allergy or irritation.
In Hyper-IgE syndrome:
-
The immune system struggles to control moulds
-
Aspergillus can behave more like a true infection, not just an allergy
-
Lung damage can happen more easily and progress faster
This means doctors may need to:
-
Monitor lungs more closely
-
Treat fungal disease earlier and for longer
-
Be cautious with repeated or long-term steroid use
Specialist centres such as the National Aspergillosis Centre are often involved when aspergillosis and immune problems overlap.
Isn’t this just severe allergy or ABPA?
Hyper-IgE syndrome can look similar to:
-
Severe allergic asthma
-
Allergic Bronchopulmonary Aspergillosis (ABPA)
The key difference is that in Hyper-IgE syndrome:
-
The immune system itself is faulty
-
High IgE is part of a wider immune problem
-
Treating allergy alone may not be enough
Some people are treated for asthma or ABPA for years before this possibility is considered.
How is Hyper-IgE syndrome treated?
There is no single cure, but good treatment can make a big difference. The aim is to prevent infections, protect the lungs, and reduce symptoms.
1. Preventing infections (most important)
Because the immune system does not fight germs normally:
-
Some people take regular low-dose antibiotics
-
Others use antibiotics early and promptly when infections start
For people with aspergillosis:
-
Antifungal medicines may be needed
-
Monitoring is usually closer and longer-term
2. Protecting the lungs
Many people develop bronchiectasis or lung damage, so care often includes:
-
Airway clearance physiotherapy
-
Saline nebulisers to help clear mucus
-
Regular sputum tests
-
Early treatment of flare-ups
The goal is to stop the cycle of:
infection → inflammation → permanent lung damage
3. Managing inflammation and allergy (carefully)
People may also have asthma-like symptoms, eczema and multiple allergies.
-
Steroids can help symptoms, but long-term or frequent use can increase infection risk
-
Doctors usually try to keep steroid doses as low as possible
Biologic treatments (such as anti-IgE medicines):
-
May help some people
-
Do not fix the immune problem
-
Are considered on an individual basis, usually in specialist centres
4. Skin care
-
Regular moisturising
-
Prompt treatment of infected eczema
-
Good skin care helps reduce infection risk
How is Hyper-IgE syndrome diagnosed?
Diagnosis usually involves:
-
A detailed review of your medical history (often including childhood infections)
-
Blood tests of immune function
-
Referral to an immunology specialist
-
Sometimes genetic testing
Does having high IgE mean I definitely have this?
No.
Hyper-IgE syndrome is rare.
But it may be worth asking about if:
-
Your IgE has always been extremely high
-
You’ve had repeated infections for many years
-
You have bronchiectasis without a clear cause
-
Aspergillosis seems unusually persistent or severe
-
Standard asthma or allergy treatments don’t fully explain your symptoms
Key message
Very high IgE does not always mean “just allergy.”
In a small number of people, it reflects a deeper immune problem that changes how aspergillosis behaves and how it should be treated.
If your illness doesn’t quite fit the usual labels, it is reasonable to ask whether an immunology review would help.
What’s New in Aspergillosis Clinical Trials (Last ~4 Months)
An overview for patients and non-specialist readers — 19 January 2026
Over the past four months, research into aspergillosis — including chronic, allergic, and invasive forms — has continued across a range of clinical trials. These studies include treatments, diagnostics, and better ways to understand who gets sick and how best to manage it.
Below is a summary of the most relevant trials now active, recruiting, or updated recently. Whenever possible, we link to the official ClinicalTrials.gov record so you can see the details, eligibility criteria, locations, and contact information.
📋 Clinical Trials of Interest
1. Phase III Olorofim Trial for Invasive Aspergillosis
Study title: Olorofim Aspergillus Infection Study
Condition: Invasive aspergillosis (IA)
What it’s testing: A new antifungal drug called olorofim compared with liposomal amphotericin B followed by standard care.
Status: Active — not currently recruiting new patients but ongoing through 2026.
Official record: Olorofim Aspergillus Infection Study on ClinicalTrials.gov
Last updated: January 4, 2026
Why this matters: Olorofim is a completely new class of antifungal designed for patients whose infection is difficult to treat with standard drugs. It may offer an alternative for those with drug-resistant or treatment-intolerant infections.
2. Rezafungin in Chronic Pulmonary Aspergillosis (CPA)
Study title: Rezafungin for Treatment of Chronic Pulmonary Aspergillosis
Condition: Chronic pulmonary aspergillosis
What it’s testing: A long-acting echinocandin antifungal (rezafungin) that might reduce dosing frequency.
Status: Recruiting / active
Official record: Rezafungin CPA Trial on ClinicalTrials.gov
Why this matters: Current CPA treatments can require daily medication and prolonged therapy. Rezafungin’s once-weekly dosing could help reduce burden and hospital visits.
3. Combination Trial: Ibrexafungerp + Voriconazole (SCYNERGIA)
Study title: Evaluate Safety and Efficacy of Ibrexafungerp With Voriconazole in Invasive Pulmonary Aspergillosis
Condition: Invasive pulmonary aspergillosis
What it’s testing: Whether combining two antifungals works better than standard therapy alone.
Status: Active (ongoing)
Official record: SCYNERGIA Combination Trial on ClinicalTrials.gov
Why this matters: Some patients don’t respond well to single-agent treatment. Combination therapy may help in severe cases, especially where resistance is a concern.
4. PCR Diagnostic Study for Aspergillus fumigatus
Study title: PCR for Aspergillus Fumigatus in Blood and Bronchoalveolar Lavage Fluid
Condition: Aspergillosis (diagnostic focus)
What it’s testing: A blood and lung fluid PCR test to improve early detection of aspergillosis.
Status: Recruiting
Official record: PCR Aspergillus fumigatus Diagnostic Trial on ClinicalTrials.gov
First posted: 2 January 2026
Why this matters: Early diagnosis increases the chance of successful treatment. A reliable PCR test could allow clinicians to start antifungal therapy sooner.
🔎 What Else Is Ongoing?
There are other studies that include aspergillosis patients or Aspergillus exposure as part of broader research, such as:
-
All-of-Us Research Program fungal infection analysis — large observational work looking at fungal disease patterns in hundreds of thousands of people in the U.S., including aspergillosis. (Not a clinical trial per se but relevant to understanding how aspergillosis affects populations.)
-
Historic or related trials — e.g., older isavuconazole comparisons (e.g., NCT00412893) exist but are not newly updated.
🧠 What This Means for Patients
-
New antifungal drugs like olorofim and rezafungin are being tested in late-stage studies — these could expand treatment options in the future.
-
Combination therapies (e.g., ibrexafungerp + voriconazole) are being assessed to tackle difficult or resistant infections.
-
Improved diagnostics (e.g., PCR tests for Aspergillus fumigatus) are now being studied to help clinicians diagnose infections earlier and more accurately.
-
Not all trials are about treatment — some focus on better ways to detect infection or understand disease patterns, which are important for prevention and clinical practice.
🗓 How to Use These Links
Clicking a trial link takes you to the official ClinicalTrials.gov page, where you can often see:
-
Who can participate
-
Locations and contact information
-
Detailed eligibility criteria
-
Sponsor and trial timelines
If you have questions about joining a trial or how it applies to you specifically, always discuss this with your healthcare team.
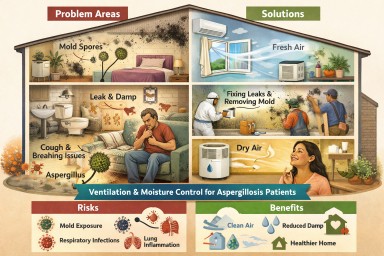
Indoor Damp, Ventilation & Aspergillosis
What a Major UK Evidence Review Means for Patients and Professionals
This large UK Health and Safety Executive (HSE) review examined whether microorganisms inside buildings (homes, offices, workplaces) can harm health — and what actually helps reduce risk.
Although it does not focus on a single disease, its findings are highly relevant to people living with aspergillosis, asthma, bronchiectasis, and other chronic lung conditions, as well as the professionals who support them.
The short answer (for everyone)
Yes — indoor environments can significantly affect lung health.
And ventilation and moisture control are central to reducing risk, especially for people vulnerable to fungal exposure.
What the review confirms (in plain language)
1. Indoor fungi are common — and not harmless
High confidence evidence
Many buildings contain airborne and surface fungi, especially when dampness is present.
The fungi most often found indoors include:
-
Aspergillus
-
Penicillium
-
Cladosporium
-
Alternaria
For aspergillosis patients, this matters because:
-
Aspergillus is not just an “outdoor mould”
-
Ongoing exposure can worsen symptoms, trigger inflammation, or complicate recovery
-
Even low levels may be problematic for sensitised or immunocompromised people
2. Dampness is a major driver of fungal exposure
High confidence
Damp buildings — whether due to leaks, condensation, or poor airflow — consistently show:
-
Higher mould growth
-
More fungal spores in the air
-
Stronger links to respiratory symptoms
Important point for patients:
You do not need to see black mould for damp to be affecting your lungs.
Mould smell (“musty odour”) is one of the strongest warning signs.
3. Ventilation is the most important protective factor
High confidence
Ventilation:
-
Dilutes fungal spores, bacteria, and viruses
-
Reduces moisture build-up
-
Lowers exposure for occupants
This applies to:
-
Homes
-
Flats
-
Offices
-
Other non-industrial indoor spaces
⚠️ The review highlights a key modern problem:
Energy-efficient, airtight buildings can unintentionally trap damp and fungi if ventilation is inadequate.
For aspergillosis patients, this means:
-
A “warm” home is not always a “healthy” home
-
Reduced airflow can increase fungal exposure even without visible mould
4. Indoor air also spreads infections
High confidence
Respiratory viruses (e.g. influenza, COVID-19) spread mainly through indoor air, especially when ventilation is poor.
This is relevant for aspergillosis patients because:
-
Viral infections can destabilise lung disease
-
Recovery may be slower
-
Secondary infections are more likely
Ventilation therefore protects against both fungal and viral risks.
5. Surfaces matter too — but air matters more
Medium–high confidence
-
Fungal material and microbes accumulate in dust, carpets, soft furnishings, and damp surfaces
-
Toilets and bathrooms can generate contaminated aerosols
-
Good hygiene helps, but cannot compensate for poor ventilation
For patients:
Cleaning alone will not solve a damp or ventilation problem.
What actually helps (evidence-based)
Strongest evidence
✔️ Adequate ventilation (natural or mechanical)
✔️ Fixing leaks and moisture sources
✔️ Removing mould-damaged materials
✔️ Preventing condensation on cold surfaces
Moderate evidence
✔️ HEPA air filtration (helpful but not a substitute for ventilation)
✔️ UV air disinfection (context-specific)
✔️ Touch-free fittings in shared buildings
⚠️ No single measure works on its own — combined approaches are needed.
Why this matters specifically for aspergillosis patients
This review strongly supports what many patients already experience:
-
Symptoms may persist despite treatment if exposure continues
-
Indoor environments can drive inflammation and relapse
-
“Just take your medication” is not enough if housing conditions are harmful
Importantly, the review recognises that:
-
Health effects vary by individual vulnerability
-
Those with asthma, bronchiectasis, aspergillosis, or immune suppression are more sensitive
-
There are no universally safe mould levels for everyone
What non-specialists should take from this
For GPs and clinicians
-
Damp and poor ventilation are legitimate medical risk factors
-
Persistent respiratory symptoms may be environment-driven
-
Asking about housing conditions is clinically relevant
For housing, environmental health & social care
-
Mould and damp are health hazards, not cosmetic defects
-
Ventilation failures can directly affect chronic disease
-
Energy efficiency must be balanced with respiratory health
For patients and carers
-
You are not “overreacting” if your home affects your breathing
-
Ventilation and moisture control are part of disease management
-
Evidence supports advocating for safer living conditions
Bottom line
This major UK review confirms that indoor dampness and poor ventilation increase exposure to fungi — including Aspergillus — and worsen respiratory health.
For people living with aspergillosis, building conditions are not secondary issues: they are part of the disease environment.

Sinusitis in Patients with ABPA
When to suspect it, when to investigate, and when to refer
Why this matters
Patients with allergic bronchopulmonary aspergillosis (ABPA) are usually managed as having a lung disease. Diagnosis, monitoring, and treatment focus appropriately on the chest, immunology, and asthma control.
However, ABPA occurs within a single continuous airway, extending from the nose and sinuses to the lungs. Disease in the upper airway can coexist with, exacerbate, or complicate lower airway inflammation — yet sinus disease is not routinely assessed in ABPA care pathways.
This article outlines:
-
What is known about sinus disease in this context
-
Which symptoms should raise suspicion
-
When investigation or ENT referral should be considered
-
What GPs and non-specialists can reasonably do
The united airway: a brief reminder
The upper and lower airways share:
-
Type 2 (eosinophilic) inflammation
-
Immunoglobulin E–mediated immune responses
-
Common triggers, including allergens and fungi
Chronic rhinosinusitis is common in asthma and severe asthma, and treatment of sinus disease can improve lower airway outcomes in some patients.
ABPA sits within this same inflammatory spectrum, even though its management is lung-centred.
Sinus disease in ABPA: what is (and isn’t) known
What we know
-
Chronic rhinosinusitis is common in patients with asthma and severe asthma
-
Sinus disease may be symptomatic or relatively silent
-
ABPA guidelines do not mandate routine ENT review or sinus imaging
-
ENT involvement, therefore, varies widely between centres
What we do not know
-
Whether routine ENT assessment improves ABPA outcomes
-
Which ABPA patients benefit most from sinus intervention
-
The optimal timing for ENT referral in ABPA
As a result, clinical judgement remains central.
Symptoms that should prompt consideration of sinus disease
Sinusitis in ABPA patients does not always present with classic “blocked nose and facial pain”.
Key symptoms include:
Common but often overlooked
-
Persistent post-nasal drip
-
Foul, bitter, metallic, or “infected” taste in the mouth
-
Throat clearing, chronic cough
-
Thick or sticky mucus sensation
-
Symptoms are worse on waking or lying flat
More typical sinonasal features
-
Nasal blockage or congestion
-
Facial pressure or fullness
-
Reduced or altered sense of smell
-
Nasal crusting or discharge
Contextual clues
-
Poor durability of response to steroids or antifungals
-
Recurrent “flares” without clear chest triggers
-
Coexisting severe asthma or nasal polyps
-
Symptoms are worse in damp or mould-affected housing
A persistent foul taste in the mouth is a recognised symptom of chronic sinus disease, usually due to post-nasal drainage of inflamed secretions.
Damp homes and sinus disease
Living in damp or mould-affected environments is associated with:
-
Higher rates of chronic rhinosinusitis
-
Upper airway irritation and inflammation
-
Allergic sensitisation to fungal spores
In most cases, this results in inflammatory or allergic sinusitis, not invasive fungal infection.
Fungal involvement may act as an immune trigger, even when not labelled as “fungal sinusitis”.
Fungal sinusitis: rare vs under-recognised
It is important to distinguish between entities:
| Type | Frequency | Key point |
|---|---|---|
| Invasive fungal sinusitis | Rare | Usually immunocompromised; dramatic presentation |
| Fungal ball (mycetoma) | Uncommon | Usually obvious on CT |
| Allergic fungal rhinosinusitis | Likely under-recognised | Requires active suspicion |
Allergic fungal rhinosinusitis overlaps biologically with ABPA:
-
IgE-mediated
-
Eosinophilic inflammation
-
Thick allergic mucin
It is not routinely sought, so it may be under-diagnosed in at-risk groups.
What GPs and non-specialists can reasonably do
1. Take upper airway symptoms seriously
Especially in ABPA or severe asthma patients with:
-
Persistent post-nasal symptoms
-
Foul taste
-
Recurrent unexplained deterioration
2. Examine the nose and throat
-
Look for polyps, discharge, and crusting
-
Note mouth breathing or altered voice quality
-
Check dentition (to exclude dental causes)
3. Consider imaging when symptoms persist
-
CT sinuses (not plain X-ray) is the imaging of choice
-
Particularly appropriate if symptoms last >8–12 weeks or recur
4. Refer to ENT when:
-
Symptoms are persistent or progressive
-
CT shows significant sinus disease
-
There is a poor response to standard medical therapy
-
There is diagnostic uncertainty
Referral does not imply surgery — ENT input may be diagnostic or medical.
What this article is not saying
-
It does not suggest that all ABPA patients need an ENT referral
-
It does not claim that sinus treatment improves ABPA outcomes
-
It does not override existing guidelines
It does suggest that earlier consideration of the upper airway is reasonable in selected patients.
Key take-home points for clinicians
-
The airway functions as a single inflammatory system
-
Sinus disease may be subtle, under-reported, or atypical
-
A foul taste in the mouth is a meaningful symptom
-
Damp or mould exposure increases sinus disease risk
-
ENT referral is appropriate when symptoms persist or recur
-
Evidence gaps remain — but clinical vigilance is justified
In summary
ABPA is managed as a lung disease, but patients live with a whole airway.
Recognising when sinus disease may be contributing can help explain persistent symptoms and guide appropriate referral — without over-investigation or over-treatment.

ABPA and Work: What a Patient Poll Tells Us About Employment, Health, and Real-World Impact
An article for patients, GPs, and non-specialist healthcare professionals
Allergic bronchopulmonary aspergillosis (ABPA) is often discussed in terms of lung function, immunology, and imaging. Far less often do we talk about its impact on everyday life, particularly on a person’s ability to work.
A poll run within the National Aspergillosis Centre patient community asked a simple but powerful question:
Who is still able to work while living with ABPA – and who has had to stop or retire?
The responses provide an important insight into the functional and socioeconomic burden of ABPA.
Key findings from the poll (patient-reported)
-
Working full time: 17%
-
Working part time (days or hours): 18% combined
-
Not working: 30%
-
Retirement age: 21%
-
Retired early for health reasons: 12%
-
Currently on sick leave / full-time carer / pre-diagnosis: small but notable groups
Even allowing for the informal nature of a social media poll, the overall pattern is clear.
What this tells us
1. Sustained full-time work is uncommon in ABPA
Fewer than one in five respondents were able to work full time. Even among those still working, many described reduced hours, flexible arrangements, or fragile employment dependent on day-to-day health.
ABPA is often incompatible with predictable, high-demand working patterns.
2. ABPA frequently leads to work loss or early retirement
A substantial proportion of respondents were either:
-
No longer working at all, or
-
Retired earlier than planned specifically because of health
This is particularly striking given that ABPA often affects people during their working years and may coexist with asthma, bronchiectasis, or long-term steroid use.
3. “Retirement age” can hide health-forced exit
Some respondents selected “retirement age,” but accompanying comments revealed that many:
-
Left work earlier than expected
-
Changed careers or reduced responsibilities years before retirement
-
Worked through ill health until they no longer could
This matters when interpreting employment statistics: health-driven work loss may be underestimated.
4. Unpaid work and instability are often overlooked
The poll also highlighted:
-
People currently on prolonged sick leave
-
Full-time unpaid carers
-
Individuals still awaiting diagnosis but already struggling to work
These groups are frequently invisible in employment data, yet represent significant personal and societal impact.
Why ABPA affects the ability to work
For patients and non-specialists, it is important to understand that work difficulties in ABPA are not simply due to “asthma symptoms.”
Common contributors include:
-
Chronic breathlessness and cough
-
Severe fatigue and post-exertional exhaustion
-
Recurrent chest infections
-
Steroid side-effects (muscle weakness, bone disease, mood changes, diabetes risk)
-
Unpredictable flare-ups requiring rest, antibiotics, or hospital care
-
Cognitive and emotional burden of long-term illness
Together, these make consistent attendance, physical work, and high cognitive load difficult to sustain.
Implications for patients
-
Difficulty working is not a personal failure
-
Many others with ABPA face similar challenges
-
Adjustments, reduced hours, or stopping work altogether may be medically appropriate
-
Asking for support is reasonable and justified
Implications for GPs and non-specialist clinicians
-
Employment status should be considered a key outcome of disease control
-
Fit notes, occupational health input, and benefits documentation are part of holistic care
-
ABPA is a fluctuating condition – patients may cope for periods and then deteriorate
-
Statements such as “lung function is stable” do not always reflect real-world functioning
Understanding the work impact helps clinicians better support patients in consultations, reports, and advocacy.
Implications for systems and policy
This poll reinforces that ABPA carries a significant socioeconomic burden, including:
-
Reduced workforce participation
-
Early retirement
-
Increased reliance on health and social support systems
Any assessment of disability, employment capability, or long-term planning must take into account:
-
Variability over time
-
Treatment burden
-
Side-effects of necessary medications
In summary
This patient poll sends a consistent message:
ABPA commonly limits the ability to work, often leading to reduced hours, unstable employment, or early exit from the workforce.
For patients, this experience is shared and valid.
For clinicians, it is a reminder that ABPA is not just a radiological or immunological diagnosis, but a life-limiting condition with real-world consequences.

Hydrocortisone dosing in adrenal insufficiency
Why adrenal insufficiency can happen in people with aspergillosis
Many people with aspergillosis, particularly those with asthma-related conditions such as allergic bronchopulmonary aspergillosis (ABPA) or more severe chronic lung disease, need treatment with steroid medicines at some point. These treatments — often essential to control inflammation, protect the lungs, and improve breathing — may include repeated or long-term courses of steroids such as prednisolone.
When steroid treatment is used over time, it can reduce the body’s own production of cortisol by the adrenal glands. In some people, the adrenal glands do not fully recover, leading to adrenal insufficiency. Cortisol is a vital hormone that helps the body manage energy, illness, infection, and physical stress. When it cannot be made reliably, hydrocortisone replacement is needed to keep the body safe and functioning.
In this situation, hydrocortisone is prescribed to replace the cortisol your body can no longer make, usually after prednisolone has been reduced or stopped, or when prednisolone is no longer needed to control lung inflammation but adrenal support is still required.
Adrenal insufficiency in people with aspergillosis is not a failure and not something you have caused. It is a recognised consequence of necessary treatment for a serious, long-term condition. With the right information, a personalised dosing plan, and medical support, adrenal insufficiency can be managed safely alongside aspergillosis.
A patient guide to everyday (basal) dosing, higher-dose needs, and short-term stress dosing
If you take hydrocortisone because you have adrenal insufficiency, understanding how your dose works — both day to day and during illness or stress — is essential for your safety and wellbeing.
This guide explains:
-
What your basal (everyday) dose is for
-
Why some people need higher basal doses
-
When and how stress dosing is used — and why it is short term
-
Why some doctors may hesitate — and how to work safely with them
-
Where to find trusted patient and clinician resources
Very important first point ❗
Any changes to your hydrocortisone dose must be agreed in advance with a doctor or specialist nurse who knows your adrenal insufficiency.
This includes:
-
Your usual daily dose
-
Your stress-dosing (“sick day”) plan
-
Emergency injection instructions
This guide does not replace medical advice.
It is designed to help you understand your treatment and communicate clearly with healthcare professionals.
1) Your basal (everyday) hydrocortisone dose
What the basal dose is for
Your basal dose is the hydrocortisone you take on an ordinary day, when you are not ill or under unusual stress. Its purpose is to:
-
Replace the cortisol your body cannot make reliably
-
Support normal daily function (energy, blood pressure, mood)
-
Help your body feel stable and safe
-
Reduce the risk of chronic under-replacement
It is replacement, not treatment for inflammation.
A key point many patients are not told
Being consistently under-replaced does not help adrenal recovery.
Ongoing symptoms such as:
-
Constant exhaustion
-
Dizziness or nausea on standing
-
Brain fog or low mood
-
Poor tolerance of everyday stress
-
Frequent “crashes” or infections
can delay recovery, not speed it. Stability supports healing.
What doctors usually mean by a “physiological” dose
Most adults naturally produce the equivalent of about 15–25 mg of hydrocortisone per day.
Doctors aim for a dose in this range and adjust for:
-
Body size
-
Activity level
-
Other medical conditions
-
Individual response
This is replacement, not “high-dose steroids”.
How basal hydrocortisone is usually taken
To mimic the body’s natural rhythm, doses are often split:
-
A larger dose in the morning
-
Smaller doses later in the day
-
Avoiding late evening doses where possible
This supports:
-
Energy and blood pressure
-
Sleep
-
Mood and concentration
Signs your basal dose may be too low
Tell your doctor if you have persistent:
-
Severe fatigue despite rest
-
“Wired but empty” feeling
-
Dizziness, nausea, or salt craving
-
Poor concentration or memory
-
Low mood or anxiety
-
Frequent need for rescue or stress doses
These symptoms matter even if blood tests look reassuring.
Blood tests are only part of the picture
Cortisol and ACTH tests:
-
Help with diagnosis
-
Are less helpful for adjusting daily dose
-
Do not always reflect how well you function
Doctors experienced with adrenal insufficiency rely heavily on how you feel and cope day to day.
The right balance
Rather than “as low as possible,” a safer aim is:
Low enough to avoid overtreatment, but high enough to live a stable, functional life.
Living in constant deficit is not success.
2) When a higher basal dose may be appropriate
Some people with adrenal insufficiency — particularly those with chronic illness — may genuinely need a higher basal hydrocortisone dose (for example 25–30 mg/day).
This does not automatically mean overtreatment.
Well-recognised examples include:
Chronic inflammatory lung disease (including ABPA)
-
Ongoing airway inflammation and immune activation
-
Recurrent infective or inflammatory flares
-
The body may never be in a true “resting” state
-
Standard doses may leave patients under-replaced
-
A stable higher dose can reduce repeated stress dosing and improve daily function
Frequent infections or slow recovery
-
Repeated illness or prolonged recovery
-
Frequent “temporary” stress dosing just to cope with everyday life
Long-standing steroid-induced adrenal insufficiency
-
Years of prednisolone or similar treatment
-
Deep suppression of the adrenal system
Larger body size or higher metabolic demand
-
Cortisol needs vary with body size and activity
Autonomic symptoms or low blood pressure
-
Postural dizziness or faintness
-
Often benefit from a higher morning dose
Clinical clue:
If someone repeatedly needs stress dosing just to manage ordinary days, their basal dose may be too low for their current physiology.
Important reassurance
-
Higher basal doses can be appropriate, temporary, or longer-term
-
They do not automatically prevent recovery
-
Ongoing inflammation and repeated physiological stress suppress recovery more than adequate replacement
-
Doses should always be prescribed, documented, and reviewed
3) Stress dosing — when your body temporarily needs more
What stress dosing means
A healthy body automatically makes more cortisol during:
-
Illness or infection
-
Fever
-
Vomiting or diarrhoea
-
Injury or trauma
-
Severe pain
-
Surgery or medical procedures
-
Major physical stress
If you have adrenal insufficiency:
➡️ your body cannot do this, so doctors prescribe stress dosing in advance as part of your safety plan.
Stress dosing is essential — but it is short term
Stress dosing is meant to last only as long as the stress lasts.
It covers a temporary increase in need, not your everyday requirements.
What “short term” usually means
Stress dosing may last:
-
24–48 hours for minor illness or fever
-
Several days for infections or recovery from injury
-
During and immediately after surgery or procedures
Your doctor should advise:
-
When to increase
-
How much to increase
-
When and how to return to your usual dose
Why stress dosing should not continue indefinitely
If higher doses are needed for longer, something usually needs review:
-
Infection or inflammation has not settled
-
The basal dose may be too low
-
Another medical problem is present
If stress dosing is still needed after the original stress has passed, it’s time to talk to your doctor.
Stepping back down safely
-
Doctors usually advise returning to baseline
-
Sometimes a 1–2 day step-down is used
-
You should not remain on stress doses “just in case”
Stress dosing does NOT:
-
Stop adrenal recovery
-
Mean you are “failing”
-
Cause long-term harm when used correctly
Not stress dosing can:
-
Make you seriously unwell
-
Delay recovery
-
Lead to adrenal crisis


4) Why some doctors seem hesitant
Doctors outside endocrinology (GPs, A&E, ward teams):
-
Are trained to minimise steroid use
-
Often think of steroids only as anti-inflammatory drugs
-
May rarely manage adrenal insufficiency
What they may not realise immediately:
Your hydrocortisone is replacing a missing hormone — it is essential, not extra.
5) How to advocate safely (with medical backing)
It is appropriate to say:
“I have adrenal insufficiency. My doctor has advised stress dosing during illness to prevent adrenal crisis.”
If you have them, show:
-
Your Steroid Emergency Card
-
A written stress-dosing plan
-
A clinic letter or summary
6) Trusted resources & further support (with links)
The following organisations provide reliable, clinician-endorsed information on adrenal insufficiency, hydrocortisone replacement, stress dosing, and emergency care.
They are widely recognised by NHS endocrinology teams and safe to share with patients, families, and healthcare professionals.
UK patient and professional resources
Addison’s Disease Self-Help Group (ADSHG)
Website: https://www.addisonsdisease.org.uk
What it offers:
-
Clear explanations of basal vs stress dosing
-
Patient-friendly sick-day rules
-
Emergency hydrocortisone injection guidance
-
Downloadable patient leaflets used in NHS clinics
-
Webinars, helpline, and peer support
Why it’s useful:
ADSHG explicitly supports individualised dosing and crisis prevention.
Society for Endocrinology
Steroid Emergency Card & adrenal crisis guidance:
https://www.endocrinology.org/clinical-practice/steroid-emergency-card/
Why it’s useful:
-
Highly trusted by doctors, A&E, and ward teams
-
Clear professional wording that reassures non-specialists
-
Supports rapid decision-making in emergencies
NHS (England)
Steroid Emergency Card information:
https://www.nhs.uk/conditions/steroid-emergency-card/
Why it’s useful:
-
Official NHS backing
-
Useful for legitimacy in emergency or inpatient settings
International patient resources (useful supplements)
Endocrine Society
Patient information on adrenal insufficiency:
https://www.endocrine.org/patient-engagement/endocrine-library/adrenal-insufficiency
Why it’s useful:
-
Clear explanations of cortisol physiology
-
Conservative, authoritative tone
-
Helpful for patients seeking international consensus
National Adrenal Diseases Foundation (NADF)
Website: https://www.nadf.us
What it offers:
-
Practical sick-day rules
-
Emergency preparedness guidance
-
Injection training resources
Particularly helpful for patients with long-standing adrenal insufficiency or frequent illness.
Resources especially relevant for ABPA & chronic lung disease
National Aspergillosis Centre
Website: https://mft.nhs.uk/wythenshawe/services/infectious-diseases/national-aspergillosis-centre/
Why it’s relevant:
-
Specialist centre where ABPA and adrenal insufficiency often overlap
-
Supports personalised care plans in complex disease
Aspergillosis Trust
Website: https://www.aspergillosistrust.org
Why it’s useful:
-
Patient-focused education and advocacy
-
Helps explain the chronic physiological stress of ABPA
-
Supports conversations about higher basal hydrocortisone needs
Quick-access patient checklist (phone / wallet)
Patients are encouraged to keep:
-
Steroid Emergency Card
-
Sick-day rules (ADSHG)
-
Personal stress-dosing plan (agreed with doctor)
-
Clinic letter or summary
Many patients keep photos of these documents on their phone for emergencies.
Final reassurance
These resources support — not replace — medical advice.
They exist to help patients stay safe, informed, and confident when managing hydrocortisone and communicating with healthcare professionals.

Season’s Greeting
As the year draws to a close, we would like to send warm wishes to everyone in the aspergillosis community — patients, families, carers, clinicians, nurses, scientists, and all professionals working to improve care and understanding.
Living with aspergillosis, or supporting those who do, often requires resilience, patience, and compassion. Throughout this year, we have seen remarkable strength from patients, dedication from healthcare teams, and generosity of spirit across our wider community.
At this time of reflection and renewal — whether you mark Christmas, another festival, or simply the turning of the year — we hope you find moments of rest, comfort, and connection. May the days ahead bring steadier health where possible, renewed energy, and continued progress in care, research, and support.
Thank you for being part of this community.
With warmest wishes for peace, kindness, and hope — now and into the New Year.

Potential respiratory hazards of fungal exposure in the residential indoor environment: a systematic review (2025)
Summary of the 2025 Systematic Review for Non-Specialists & Patients
Read full paper here: Potential respiratory hazards of fungal exposure in the residential indoor environment: a systematic review - ScienceDirect
What was this review about?
This review looked at all the scientific evidence from 1990–2025 on how indoor fungi (moulds) in homes affect people’s breathing and general respiratory health. It examined 94 studies, mapping out where fungi come from, which species appear most often, and how they affect the lungs, nose, throat, and immune system.
Key Findings in Plain Language
1. The biggest sources of indoor mould are dampness and building damage
Homes with water leaks, damp walls, damaged materials and poor ventilation are the most common sources of fungi—especially Aspergillus and Penicillium. These thrive in wet building materials, bathrooms, kitchens, drains, air-conditioning systems and even water dispensers.
2. Indoor fungi are strongly linked to a wide range of respiratory symptoms
Across many countries, indoor fungal exposure was associated with:
-
Asthma and asthma flare-ups
-
Allergic rhinitis (blocked or runny nose)
-
Chronic cough and throat irritation
-
Adenoid enlargement in children
-
Hypersensitivity pneumonitis (allergic inflammation of the lungs)
-
Reduced lung function
-
Even pulmonary haemorrhage in rare cases
The review shows that even everyday exposure—not just visibly mouldy homes—can worsen respiratory health.
3. Some fungi are more strongly associated with illness
Important associations include:
-
Aspergillus → asthma symptoms, COPD exacerbations, throat irritation, hypersensitivity reactions
-
Penicillium → asthma, allergic rhinitis, hypersensitivity pneumonitis
-
Alternaria → childhood asthma risk
-
Candida & Fusarium → present in wet areas such as bathrooms and may affect vulnerable individuals
4. The geographic picture is uneven
Most research comes from high-income, temperate countries. There are major evidence gaps in tropical and subtropical regions, where humidity is high and fungal exposure is likely worse. This limits current global understanding of risk.
5. Prevention works — but public awareness is low
Simple actions (cleaning, improved ventilation, addressing leaks, correct humidity ranges) can radically reduce fungal burden. One study showed 80–90% reduction in airborne mould counts after residents were given basic remediation advice.
What’s New or Important in This 2025 Review?
1. A fully integrated “source → species → disease → location” map
The review is the first to link fungal sources, the exact fungi found, the diseases they cause, and where the evidence comes from, creating a multi-layered evidence map. This helps identify:
-
Which household features pose the highest risk
-
Which fungi are clinically most important
-
Where research gaps exist
2. Highlights the major global research imbalance
It emphasises that very little evidence exists from low-income and tropical areas—where exposure may be far more severe. This is a call for equity and better global surveillance.
3. Shows that fungi may affect more than the lungs
The review notes new evidence that fungal exposure may also influence neurological and immune-mediated symptoms, suggesting mould exposure could have broader health effects than traditionally recognised.
4. Identifies major gaps in identifying which fungal species cause harm
Many studies only measure “mould level” without identifying the fungus. The review argues for better fungal detection technologies, such as:
-
Portable real-time samplers
-
Multi-omics (DNA, RNA, metabolites)
-
Long-term cohort studies
These tools could finally clarify which fungi cause which illnesses.
5. Strong emphasis on emerging technologies for prevention
Including:
-
UV and photocatalytic TiO₂ devices
-
Improved antifungal cleaning agents
-
Building materials designed to resist mould growth
-
Volcanic minerals and clays that absorb harmful compounds
Why This Review Matters (for Patients, Carers, and Clinicians)
1. It shows mould is not “just an allergy problem”
Indoor fungi can worsen or trigger asthma, COPD, hypersensitivity pneumonitis, chronic sinus issues, and may even influence immune and neurological health. This validates patient experiences where damp homes worsen symptoms.
2. It provides strong evidence for housing-related health advocacy
Patients can use this to:
-
Request landlord repairs
-
Support home assessments
-
Advocate for rehousing if severe mould is present
-
Justify humidifier/dehumidifier use, and ventilation improvements
3. It highlights the importance of early remediation
Even simple cleaning and remediation steps can dramatically reduce mould burden and symptoms—important for families, vulnerable groups, and those with chronic lung disease.
4. It gives clinicians a clearer evidence base
Respiratory teams can use this to:
-
Recognise when housing contributes to disease flare-ups
-
Understand which conditions are most strongly linked to indoor fungi
-
Make better-informed referrals for environmental health assessments
5. It builds a scientific foundation for future guidelines
The authors point out that national building codes, indoor air quality policies, and public health guidance lag behind the evidence—and this review is intended to inform future regulation.
Who Does This Help Most?
Patients with:
-
Asthma
-
Allergic bronchopulmonary aspergillosis (ABPA)
-
Aspergillus bronchitis
-
COPD (especially those with fungal-associated exacerbations)
-
Hypersensitivity pneumonitis
-
Children with recurrent respiratory infections
-
Anyone living in damp, mouldy, water-damaged, or poorly ventilated homes
Clinicians:
Respiratory physicians, GPs, ENT specialists, allergists, immunologists.
Policy & Housing Professionals:
Public health teams, environmental health officers, social landlords, housing associations.
Researchers:
Those developing diagnostics, fungal exposure studies, indoor air quality monitoring, or patient-centred environmental interventions.

Aspergillosis Patient Conference 2025 – summary and recording

The Aspergillosis Patient Conference 2025 took place online on 29 November 2025. The event was co-organised and co-presented by the National Aspergillosis Centre (NAC) and The Aspergillosis Trust, in collaboration with the European Lung Foundation (ELF).
The free conference brought together people living with aspergillosis, carers, patient advocates, clinicians and researchers from across Europe and beyond. Its focus was firmly patient-centred, combining clinical expertise with lived experience to improve understanding, awareness and care.
🎥 The full conference recording is now available to watch online, enabling anyone who missed the live event to benefit from the sessions and discussions.
What the conference covered
Across the programme, speakers explored:
-
What aspergillosis is and the different forms it can take
-
Symptoms and diagnostic challenges, including delays in recognition
-
Current treatment and management approaches
-
Living with aspergillosis, shared directly by patients
-
What needs to improve, including awareness, education and access to specialist care
Live questions, polling and discussion ensured that patient priorities and real-world concerns shaped the conversation throughout.
Speakers and perspectives
The conference featured a broad range of patient advocates and clinical experts, including:
-
People with lived experience of chronic pulmonary aspergillosis (CPA) and allergic bronchopulmonary aspergillosis (ABPA)
-
Representatives from NAC, The Aspergillosis Trust and the ELF Aspergillosis Patient Advisory Group
-
Respiratory physicians, infectious disease specialists and researchers involved in European clinical guidelines and research
This mix ensured that sessions reflected both medical best practice and day-to-day patient realities.
Who the recording is useful for
The on-demand recording is particularly valuable for:
-
People living with aspergillosis and related lung conditions
-
Family members, carers and supporters
-
Healthcare professionals seeking a patient-focused overview
-
Patient organisations and advocates working in respiratory or fungal disease
Why this conference matters
Aspergillosis remains under-diagnosed and poorly understood, despite its significant impact on health and quality of life. This conference highlighted:
-
The importance of patient voices in education and guideline development
-
The need for earlier diagnosis and clearer care pathways
-
The value of collaboration between specialist centres, patient charities and European organisations
By making the recording freely available, NAC, The Aspergillosis Trust and ELF have ensured the conference continues to support patients, carers and professionals well beyond the live event.