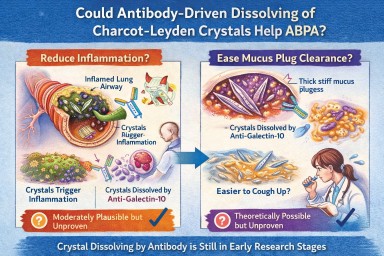
🧬 Could Antibody-Driven Dissolving of Charcot–Leyden Crystals Help ABPA?
Researchers have recently discovered that Charcot–Leyden crystals (CLCs) — the needle-shaped structures formed from the eosinophil protein galectin-10 — are not just debris.
In laboratory studies, specially designed antibodies can dissolve these crystals.
This has raised two important questions:
-
Could dissolving the crystals reduce airway inflammation?
-
Could dissolving them make mucus plugs easier to clear?
Here is what we currently know.
1️⃣ Could dissolving crystals reduce airway inflammation?
What we know
Laboratory and animal studies have shown:
-
Charcot–Leyden crystals can activate immune cells (especially macrophages).
-
They can stimulate inflammatory pathways (including inflammasome signalling).
-
In mouse models, antibodies targeting galectin-10 dissolved the crystals.
-
When crystals were dissolved, airway inflammation decreased.
This suggests that the crystals themselves may amplify inflammation, rather than simply mark it.
What this means biologically
In ABPA and eosinophilic asthma:
-
Eosinophils release galectin-10.
-
Galectin-10 crystallises.
-
Crystals may trigger further immune activation.
-
That leads to more inflammation → more eosinophils → more crystals.
Dissolving the crystals could theoretically interrupt this feedback loop.
How likely is this to help inflammation in humans?
Moderately plausible, but not yet proven.
The biological mechanism is strong.
The animal data are encouraging.
But no human clinical trials have yet shown reduced inflammation through crystal dissolution.
If developed successfully, this approach could:
-
Reduce airway immune activation
-
Lower exacerbation risk
-
Potentially reduce steroid dependence
But at present, it remains investigational.
2️⃣ Could dissolving crystals make mucus plugs easier to cough up?
This is more speculative — but still biologically reasonable.
Why mucus plugs are so thick in ABPA
ABPA mucus plugs contain:
-
Gel-forming mucins
-
DNA from inflammatory cells
-
Dead cells
-
Fungal fragments
-
Eosinophil proteins
-
Charcot–Leyden crystals
The crystals are:
-
Rigid
-
Needle-shaped
-
Structurally stable
When embedded in mucus, they likely increase:
-
Mechanical stiffness
-
Plug density
-
Resistance to deformation
From a physics perspective:
Removing rigid crystalline structures from a gel should reduce stiffness and improve flow.
Do we have direct evidence?
No.
There are currently:
-
No human studies measuring mucus clearance after crystal dissolution
-
No trials showing improved plug expectoration from crystal-targeting therapy
So while it is plausible that dissolving crystals could soften plugs, this has not yet been demonstrated in patients.
3️⃣ How strong is the overall case?
| Outcome | Evidence strength | Likelihood |
|---|---|---|
| Reduced inflammation | Strong biological rationale + animal data | Moderately promising |
| Easier mucus clearance | Biophysical plausibility only | Possible but unproven |
Inflammation reduction is the more evidence-supported target.
Improved plug clearance is plausible but currently theoretical.
4️⃣ How does this compare to existing treatments?
Current therapies (e.g., anti-IL-5 biologics) reduce eosinophils upstream.
That leads to:
-
Less galectin-10 release
-
Fewer crystals forming
-
Reduced inflammation
-
Often improved mucus plugging
So biologics already indirectly reduce crystal burden.
A crystal-dissolving antibody would act downstream, targeting the structural product directly.
This could theoretically:
-
Accelerate resolution of existing plugs
-
Reduce residual inflammatory signalling
But again, this remains in early research stages.
5️⃣ Practical take-home message
At present:
-
Dissolving Charcot–Leyden crystals reduces inflammation in animal models.
-
It is biologically plausible that this could also soften mucus plugs.
-
There is no human clinical proof yet.
-
No approved therapy currently targets the crystals directly.
The concept is scientifically credible — but still under development.
🔭 The Bigger Picture
ABPA is increasingly understood as a condition driven by:
-
Eosinophils
-
Allergic immune signalling
-
Abnormal mucus biology
-
Structural plug formation
Crystal-targeting therapies may eventually become part of a more precise approach to treating eosinophilic airway disease.
But for now, they remain a promising research direction rather than a clinical option.
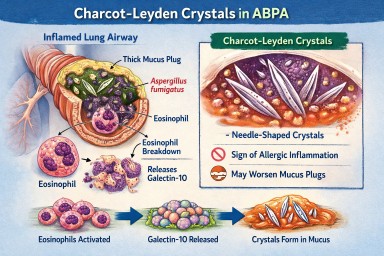
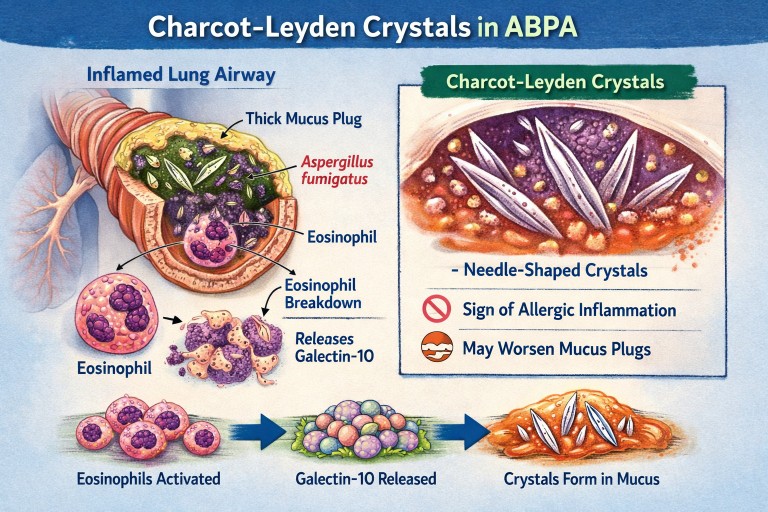
🔬 Charcot–Leyden Crystals in ABPA and Asthma
What are they? Why do they form? Do they matter?
If you live with Allergic Bronchopulmonary Aspergillosis (ABPA) or severe asthma, you may see the term Charcot–Leyden crystals in a sputum or pathology report.
They can sound worrying.
They are:
-
Not fungus
-
Not infection
-
Not cancer
They are a sign of a particular type of allergic inflammation in the airways.
🧬 What Are Charcot–Leyden Crystals?
Charcot–Leyden crystals are microscopic, needle-shaped structures found in mucus.
They are made from a protein called galectin-10, which is stored inside a type of white blood cell called an eosinophil.
Eosinophils are immune cells involved in:
-
Allergic asthma
-
ABPA
-
Severe asthma with fungal sensitisation
-
Parasitic infections
When eosinophils are activated and break down, they release galectin-10.
If enough of this protein accumulates in thick airway mucus, it crystallises into visible crystals.
So the crystals are made from your immune cells, not from Aspergillus.
🫁 Why Do They Appear in ABPA?
In ABPA:
-
The immune system overreacts to Aspergillus fumigatus.
-
This triggers a strong allergic (Type 2) immune response.
-
Large numbers of eosinophils move into the airways.
-
Eosinophils break down and release galectin-10.
-
The protein crystallises inside mucus plugs.
The crystals are therefore a footprint of intense allergic inflammation, not fungal invasion.
🌡 Is Most ABPA Eosinophilic?
Yes — almost all classical ABPA is eosinophilic.
ABPA is fundamentally a Type 2 allergic condition, driven by immune pathways involving:
-
IL-4
-
IL-5
-
IL-13
-
IgE
-
Eosinophils
IL-5 in particular stimulates eosinophil production and survival.
Because of this, eosinophils are central to the disease process.
Historically, raised blood eosinophils have been part of diagnostic criteria.
However:
-
Eosinophil counts can fluctuate
-
Steroids can suppress blood levels
-
Eosinophils may still be present in airway mucus even if blood counts appear normal
So ABPA is biologically eosinophilic — even if a single blood test does not show a high count.
True non-eosinophilic ABPA would be unusual and would prompt clinicians to reconsider the diagnosis.
❓ Are Crystals Caused by Aspergillus Infection?
No.
They are caused by the immune reaction to Aspergillus — not by the fungus itself.
They can also be seen in:
-
Severe eosinophilic asthma
-
Parasitic infections
-
Other allergic lung conditions
They reflect eosinophil activity, not fungal growth.
🧠 Why Don’t All People with Asthma Develop These Crystals?
Asthma is not one single disease. It has different inflammatory patterns.
Type 2 (Eosinophilic) Asthma
This involves high eosinophils and allergic pathways.
Common in:
-
Allergic asthma
-
ABPA
-
Severe eosinophilic asthma
These patients can develop Charcot–Leyden crystals.
Non–Type 2 (Non-Eosinophilic) Asthma
This includes:
Neutrophilic asthma
Driven by neutrophils rather than eosinophils.
Paucigranulocytic asthma
Very few inflammatory cells present.
In these forms:
-
Eosinophils are low
-
Galectin-10 is not released in large amounts
-
Crystals are unlikely to form
🧱 Do Charcot–Leyden Crystals Make Mucus Plugs Worse?
Possibly.
Research suggests they may:
-
Increase mucus thickness
-
Contribute mechanically to airway blockage
-
Stimulate further inflammation
For many years they were thought to be harmless debris.
Modern studies suggest they may actively amplify inflammation when present in large amounts.
🎯 Do They Have a Purpose?
Eosinophils evolved mainly to help fight parasitic infections.
Galectin-10 probably has immune signalling roles inside cells.
However, when large amounts are released into thick airway mucus, crystallisation appears to be a by-product of excessive immune activity rather than a useful defence.
In ABPA and allergic asthma, they are more likely part of the problem than part of the solution.
💧 Can Their Formation Be Reduced?
Hydration alone does not stop them forming.
Drinking fluids helps:
-
Keep mucus less sticky
-
Support airway clearance
But it does not prevent eosinophils releasing galectin-10.
What reduces crystal formation?
Reducing eosinophilic inflammation:
-
Corticosteroids
-
Anti-IL-5 biologics
-
Anti-IL-4/IL-13 biologics
When eosinophil numbers fall:
→ Less galectin-10 is released
→ Fewer crystals form
Antifungal treatment in ABPA may indirectly help by reducing allergic stimulation, but the main driver is the immune response.
📊 Do They Change Treatment?
Not directly.
Doctors base treatment on:
-
Symptoms
-
Blood eosinophils
-
Total IgE
-
Imaging
-
Lung function
-
Exacerbation history
Crystals support the diagnosis of eosinophilic inflammation but do not determine treatment alone.
🔎 What Do They Tell Us?
Charcot–Leyden crystals tell us:
-
The airway inflammation is eosinophilic.
-
The immune response is strongly allergic.
-
Mucus plugging risk may be higher.
They are a marker of immune overreaction, not infection severity.
🧠 Key Points to Remember
-
They are made from proteins released by eosinophils.
-
They are not Aspergillus.
-
They do not mean invasive fungal infection.
-
Most classical ABPA is eosinophilic.
-
They are unlikely in non-eosinophilic asthma.
-
Reducing eosinophils reduces their formation.
-
Hydration helps clearance but does not prevent formation.
In simple terms:
Charcot–Leyden crystals are microscopic signs that the immune system is working too hard in the airways.
Event: 📸 Science is Open: A Photo Journey of Research Lab Samples
Have you ever wondered what happens to samples used in research?
The KHP Centre for Translational Medicine is inviting people living with a lung condition to take part in a unique behind-the-scenes experience:
Science is Open: A Photo Journey of Research Lab Samples
This is a rare opportunity to:
-
Go inside a working research laboratory
-
Learn how lung samples are processed and studied
-
Capture the experience through photography
-
Help tell the story of research from a patient perspective
📍 When and Where?
Date: Monday 16th February
Time: Afternoon (exact timing provided after registration)
Location: Central London – Lab tour at Guy's Hospital (London Bridge)
🔬 On the Day You Will:
-
Tour a research lab at Guy’s Hospital
-
Hear directly from researchers about how lung tissue samples are handled and studied
-
Take photographs during the visit (you will be provided with a simple, easy-to-use camera)
-
Receive guidance from a professional photographer
-
Help create a visual story to share with other lung health communities
No previous research or photography experience is needed — just bring yourself.
💷 Reimbursement
-
Travel expenses will be covered
-
Payment for your time: £27.50 per hour (NIHR standard rate)
✉ How to Express Interest
To register your interest, please email Emily and include:
-
A few sentences about your experience with lung health
-
Why you would like to be involved
-
Why you feel your perspective is important
Email Emily to express your interest.
Places are limited and events like this do not come around often.
🌍 Other Opportunities
The team are also running similar events for people living with:
-
Cancer
-
Arthritis
-
Cardiovascular conditions
-
Child and maternal health conditions
If any of these areas are of interest to you, your friends, or family members, please contact Emily for further details.
Event organised by the KHP Centre for Translational Medicine
Shared with thanks to Catherine, Senior Research Impact Officer, Asthma + Lung UK.

How to Join Our Microsoft Teams Meetings - Troubleshooting

(For patients, carers and external guests)
You do not need a Microsoft account to join.
Most people can join easily using their internet browser.
✅ The Easiest Way to Join (Laptop or Desktop)
-
Click the meeting link we sent you.
-
When prompted, choose:
“Continue in this browser”
(You do NOT need to download Teams.) -
Type your name.
-
Click Join now.
-
If asked, allow access to your microphone and camera.
Please wait in the lobby until we admit you.
📱 Joining on a Phone or Tablet
-
Tap the meeting link.
-
If you already have the Microsoft Teams app, it will open automatically.
-
If not, you can download the free Teams app from your app store.
-
Enter your name and join.
Phones often work even if laptops have problems.
⚠️ If You Are Asked to Sign In
You do not need to sign into Microsoft.
If you see a sign-in screen:
-
Look for “Join as guest”
-
Or close the page and reopen the link
-
Or choose “Continue in this browser”
Avoid signing in with a work or NHS account unless you are sure it allows external meetings.
🔧 If It Doesn’t Work on Your Laptop
Try one of these:
-
Open the link in a Private / Incognito window
-
Try a different browser (Chrome or Edge usually work best)
-
Make sure you are not already signed into multiple Microsoft accounts
If you are using a work or NHS laptop, security settings may block external meetings. In that case:
👉 Try your personal laptop or your phone.
🎤 Audio & Camera Tips
-
If your microphone does not work, leave the meeting and rejoin.
-
If you prefer, you can turn your camera off.
-
You can also use the chat box to type questions.
📞 Still Having Trouble?
If you cannot join:
-
Try using your phone instead.
-
Or contact us before the meeting and we will help where we can.
Systemic fungal infections: why speed, diagnosis and stewardship matter
Systemic fungal infections — including aspergillosis, candidiasis, cryptococcosis, mucormycosis and pneumocystis pneumonia — are medical emergencies. When diagnosis or treatment is delayed, mortality rises sharply. This comprehensive review brings together current understanding of how these infections arise, why they are so difficult to diagnose, and what is needed to improve outcomes.
Why fungal infections are often missed
Unlike many bacterial infections, systemic fungal infections can be hard to confirm quickly. Fungal organisms are often present in low numbers, may be released intermittently into the bloodstream, and can be difficult to grow in standard cultures. As a result, no single test is usually sufficient, and clinicians often need a combination of imaging, cultures, antigen tests, molecular tests (PCR), and histopathology.
Because delay can be fatal, antifungal treatment is frequently started on clinical suspicion alone — especially in critically ill or immunocompromised patients. The paper emphasises that this approach is often necessary, but it must be paired with a clear diagnostic strategy.
Antifungal stewardship: knowing when to stop
A central message of the paper is that diagnostic tests are just as important for stopping treatment as for starting it. Antifungal drugs can be toxic, interact with many other medicines, and drive antifungal resistance if used unnecessarily.
The authors stress that:
-
Diagnostic results should be actively reviewed
-
Antifungal therapy should be stopped or stepped down if infection is not supported by evidence
-
This approach protects patients and preserves antifungal effectiveness
Antifungal resistance is a growing threat
Antifungal resistance is no longer rare. The review highlights:
-
Azole resistance in Aspergillus, including cryptic species
-
Rising resistance in several Candida species
-
The global spread of multidrug-resistant Candida auris
Because of this, the authors recommend that all clinically relevant fungal isolates are identified to species level and tested for antifungal susceptibility wherever possible. Making assumptions about drug sensitivity is increasingly unsafe.
Aspergillosis: a broad spectrum of disease
The paper clearly outlines the many forms of aspergillosis, ranging from:
-
Allergic disease (such as allergic bronchopulmonary aspergillosis)
-
Chronic pulmonary aspergillosis, often in people with underlying lung damage
-
Subacute and acute invasive disease, particularly in immunocompromised or critically ill patients
Importantly, the review notes that aspergillosis is not limited to severely immunocompromised people. Chronic and subacute forms often occur in individuals with structural lung disease who are otherwise immunocompetent.
Climate change and emerging fungal risks
One of the most forward-looking sections of the paper addresses how climate change and natural disasters are altering fungal disease patterns. Rising environmental temperatures, flooding, storms and environmental disruption are:
-
Increasing exposure to environmental fungi
-
Enabling fungi to adapt to higher temperatures
-
Contributing to outbreaks after natural disasters and trauma
-
Expanding fungal diseases into new geographic regions
The authors argue that fungal infections must be considered part of future public health and healthcare resilience planning.
Key take-home messages
-
Systemic fungal infections are time-critical medical emergencies
-
Diagnosis usually requires multiple tests, not a single result
-
Early antifungal treatment is often necessary — but must be reviewed
-
Diagnostics are essential for safe antifungal stewardship
-
Antifungal resistance is a real and growing problem
-
Climate change is reshaping fungal epidemiology and risk
Free access to the full article
Elsevier has provided free access to the full paper for a limited time (no registration required):
👉 https://authors.elsevier.com/a/1mZqR4qdNoJLH2
🗓️ Available until 28 March 2026
This article is recommended reading for patients wanting a deeper understanding of fungal disease, as well as clinicians, microbiology teams, and healthcare planners.

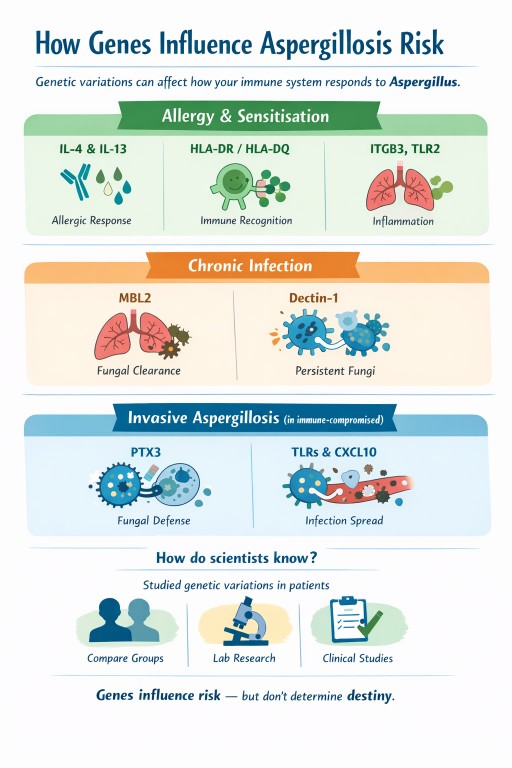
Genes and aspergillosis: why the same fungus causes different problems in different people
Why look at genes when talking about aspergillosis?
The theme of World Aspergillus Day 2026 was “How can the genomics revolution help patients with chronic aspergillosis?”
To answer that, we need to look briefly at genes and what they tell us about how the body resists infection.
Genes are the body’s instruction manual. They help control how our immune system works, how inflammation is managed, and how well we clear infections. Humans have around 25,000 genes, with two copies of each in almost every cell — and billions of cells using these instructions every day.
Small, natural differences in genes help explain why people respond differently to Aspergillus: some develop allergy, others chronic infection, and many clear it without any illness at all. Genes don’t determine outcomes, but they help us understand why the immune response differs between people.
Many people ask an understandable question:
“If we all breathe in Aspergillus spores, why do only some people get aspergillosis – and why does it look so different from person to person?”
Part of the answer lies in genes.
Genes do not cause aspergillosis on their own, but they can influence how the immune system responds once the fungus is encountered.
A simple way to think about genes
Genes act like settings, not switches.
They can influence:
-
how strongly your immune system reacts
-
whether that reaction is allergic, chronic, or weak
-
how well fungi are cleared from the lungs
Genes do not override:
-
lung damage (asthma, bronchiectasis, old infections)
-
steroid or immunosuppressive treatment
-
mould exposure levels
They help explain patterns of illness, not certainty.
Risk stacking: why combinations matter more than any single factor
Aspergillosis rarely develops because of one single cause. Instead, it usually arises through risk stacking, where several small risk factors overlap at the same time.
Each factor may add only a little vulnerability on its own, but together they can tip the balance from resistance to disease.
This helps explain why aspergillosis often appears after years of stability, or during periods of change such as illness, medication adjustment, or increased environmental exposure.
What does risk stacking look like in practice?
A person might have:
-
mild genetic tendencies toward allergic inflammation or reduced fungal clearance
-
asthma, bronchiectasis, or old lung damage
-
long-term inhaled or oral corticosteroid treatment
-
periods of higher mould exposure (for example, damp housing or renovation work)
None of these alone guarantees illness.
But stacked together, they increase the chance that Aspergillus:
-
is recognised as an allergen rather than ignored
-
is not cleared efficiently from the lungs
-
triggers ongoing inflammation or chronic infection
Where genes fit into risk stacking
Genes usually act as background modifiers, not primary causes.
In people with healthy lungs and normal immunity, genetic differences rarely matter.
In people who already have lung disease, immune suppression, or repeated exposure, those same genetic differences can add to the overall risk stack.
This also explains why there is no single genetic test that can predict aspergillosis — risk depends on combinations, not on one gene.
Just as risks can add up, risk reduction also adds up. Improvements in airway clearance, asthma control, steroid management, and home environment can all meaningfully reduce overall risk.
Why this matters in aspergillosis
Aspergillosis is not one condition. It includes:
-
fungal sensitisation and allergy
-
chronic pulmonary infection
-
invasive disease in people with weakened immunity
Different genes influence different stages of the immune response, which helps explain why people experience very different forms of disease.
1. Genes linked to fungal allergy and sensitisation
These genes affect whether the immune system treats Aspergillus as a strong allergen.
IL-4, IL-13 and the IL-4 receptor
What they do
Control allergic inflammation, including:
-
immunoglobulin E (IgE)
-
eosinophils
-
mucus production
-
airway inflammation
What this means
Certain natural gene variants increase the likelihood of:
-
fungal sensitisation
-
asthma with fungal sensitisation
-
allergic bronchopulmonary aspergillosis (ABPA)
This fits closely with what patients experience clinically: high IgE, eosinophilia, steroid responsiveness, and response to biologic treatments.
HLA-DR and HLA-DQ
What they do
Help the immune system decide which proteins deserve attention.
What this means
Some HLA types present Aspergillus proteins in a way that:
-
encourages persistent allergic inflammation
-
increases the chance of ABPA
This helps explain why only a minority of people with asthma develop ABPA.
ITGB3 (integrin beta-3)
What it does
Helps airway and immune cells:
-
attach to surrounding tissue
-
communicate danger signals
-
interact with fungal-recognition pathways
What this means
Certain versions are linked to:
-
mould sensitisation
-
stronger immune signalling when fungal particles are present
This does not mean ITGB3 causes aspergillosis.
It helps explain why some people become sensitised more easily.
TLR2
What it does
Recognises fungal cell-wall components and triggers early immune responses.
What this means
Different versions can amplify or dampen inflammation, influencing sensitivity to fungi.
2. Genes linked to chronic pulmonary aspergillosis (CPA)
These genes influence how well fungi are cleared, especially in damaged lungs.
MBL2 (mannose-binding lectin)
What it does
Marks fungi so the immune system can remove them.
What this means
Low MBL activity may allow Aspergillus to persist once lung cavities or scarring exist.
Dectin-1 (CLEC7A)
What it does
Detects fungal cell-wall sugars and triggers antifungal responses.
What this means
Reduced detection can allow slow, long-term infection rather than allergy.
TLR4
What it does
Regulates inflammation in response to microbes.
What this means
Certain variants may influence how chronic inflammation and tissue damage evolve.
3. Genes linked to invasive aspergillosis
These matter most in people with weakened immune systems (for example, during chemotherapy or after transplant).
PTX3 (pentraxin-3)
What it does
Acts as an early fungal sensor and helps immune cells kill Aspergillus.
What this means
Reduced PTX3 activity is one of the strongest known genetic risk factors for invasive aspergillosis in high-risk medical settings.
TLR3 and interferon pathways (including CXCL10)
What they do
Coordinate immune communication and antifungal killing.
What this means
Impairment can delay fungal control and increase the risk of spread.
How do scientists know these genes are involved?
Researchers study natural genetic variations that:
-
are common in healthy people
-
are present from birth
-
usually cause small functional differences, not disease by themselves
They:
-
compare people with aspergillosis to similar people without it
-
identify gene variants linked to specific disease patterns
-
test how those genes affect fungal recognition, inflammation, or killing
-
confirm findings in laboratory and clinical studies
These are risk modifiers, not disease-causing genes.
Does this mean my family is at risk?
This is a very common concern. The reassuring answer for most people is:
No – aspergillosis does not usually run in families.
Why this is reassuring
-
These gene variants are common in the general population
-
Most people who carry them never develop aspergillosis
-
Aspergillosis requires other factors, such as lung disease, immune suppression, or heavy exposure
-
There is no consistent pattern of aspergillosis being passed from parent to child
Even strong genetic signals (such as PTX3) only increase risk in specific high-risk medical situations, not in healthy relatives.
Putting it all together
| Pattern of disease | Genes most often involved |
|---|---|
| Fungal sensitisation | IL-4, IL-13, IL-4 receptor, ITGB3, TLR2 |
| ABPA | IL-4/IL-13 pathway, HLA-DR/DQ, TLR3 |
| Chronic pulmonary aspergillosis | MBL2, Dectin-1, TLR4 |
| Invasive aspergillosis | PTX3, interferon pathways |
What this means for patients and families
-
Genetic testing is not routinely needed
-
These genes do not predict individual outcomes
-
Family members are not usually at increased risk
The most important factors remain:
-
good lung care
-
appropriate treatment
-
sensible mould exposure reduction
Genes influence risk — they do not determine destiny.
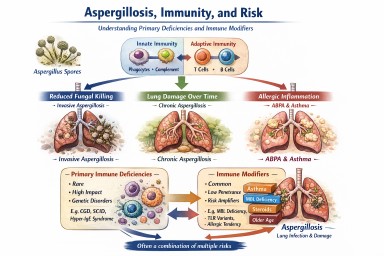
Aspergillosis, immunity, and risk
Primary immune deficiencies and immune modifiers explained
A single, comprehensive explainer for expert patients, carers, and non-specialists
Why this article exists
Aspergillus is a mould that everyone breathes in every day. Most people clear it without difficulty.
A small number of people develop aspergillosis because the balance between the fungus, the lungs, and the immune system is disturbed.
This article explains:
-
Rare primary (inherited) immune deficiencies that are clearly linked to aspergillosis
-
Common immune “modifier” factors that can increase risk or severity but do not cause disease on their own
-
How these factors stack together in real life
Key reassurance up front
There are 500+ recognised primary immune deficiencies
Only ~20–30 are clearly linked to aspergillosis
Most people with aspergillosis do not have any inherited immune disorder
The unifying concept: three immune pathways to aspergillosis
Almost all immune–aspergillus relationships fall into three mechanisms. Understanding these matters more than memorising names.
1. Reduced ability to kill the fungus
Some immune cells fail to destroy Aspergillus spores effectively.
→ Risk of invasive aspergillosis, sometimes severe or life-threatening.
2. Lung damage over time
Repeated infections or inflammation damage airways or leave cavities.
→ Risk of chronic pulmonary aspergillosis (CPA) or aspergillomas.
3. Excessive allergic inflammation
The immune system over-reacts to Aspergillus rather than failing to fight it.
→ Allergic bronchopulmonary aspergillosis (ABPA) and severe fungal-sensitised asthma.
Many conditions overlap more than one pathway.
Section 1: Primary (inherited) immune deficiencies clearly linked to aspergillosis
Rare, high-impact, and sometimes life-changing when present
These are the conditions clinicians usually mean when they talk about “immune causes of aspergillus disease”.
A. Phagocyte defects
Strongest association with invasive aspergillosis
-
Chronic granulomatous disease (CGD)
-
Autosomal recessive forms of CGD
-
Severe congenital neutropenia
-
Cyclic neutropenia
-
Leukocyte adhesion deficiency type I
Typical pattern
-
Aspergillosis at a young age
-
Invasive lung disease ± spread beyond lungs
-
Often no other obvious risk factors
B. Hyper-IgE and severe allergy syndromes
Allergic, chronic, and cavity-associated disease
-
STAT3 hyper-IgE syndrome
-
DOCK8 deficiency
-
PGM3 deficiency
-
ZNF341 deficiency
-
IL6ST deficiency
Typical pattern
-
Severe asthma and allergy
-
Thick mucus, recurrent infections
-
ABPA, later CPA or aspergillomas
C. Combined immunodeficiencies
Immune coordination problems
-
Severe combined immunodeficiency (milder or surviving forms)
-
Omenn syndrome
-
ZAP-70 deficiency
-
Major histocompatibility complex class II deficiency
-
CD40 ligand deficiency (hyper-IgM syndrome)
Typical pattern
-
Broad infection susceptibility
-
Aspergillosis can behave aggressively
D. Defects of fungal recognition and innate signalling
Often dramatic or unexpected presentations
-
CARD9 deficiency
-
Dectin-1 (CLEC7A) complete deficiency
-
MALT1 deficiency
Typical pattern
-
Severe or unusual aspergillosis
-
Lung, brain, or deep tissue involvement
-
Sometimes first presents in adulthood
E. Immune dysregulation syndromes
Mixed infection, inflammation, and autoimmunity
-
CTLA-4 haploinsufficiency
-
LRBA deficiency
-
STAT1 gain-of-function mutations
-
IPEX syndrome (FOXP3 deficiency)
Typical pattern
-
Inflammatory lung disease
-
Chronic or invasive aspergillosis emerging over time
F. Antibody deficiencies (indirect risk via lung damage)
-
Common variable immunodeficiency
-
X-linked agammaglobulinaemia
-
Activated PI3K-delta syndrome
Important nuance
Antibodies do not normally kill Aspergillus.
Risk arises after years of lung damage, not early in life.
Section 2: Immune modifier-types that can amplify risk
Common, low-penetrance, and often invisible on routine testing
These are not immune deficiencies, but they can influence who struggles, how severely, and why disease persists.
Mannose-binding lectin (MBL) deficiency
-
Common (≈5–10% of population)
-
Affects fungal recognition and complement activation
-
Usually mild on its own
-
Becomes relevant with lung disease, steroids, or other immune issues
Partial fungal-recognition receptor variants
-
Heterozygous dectin-1 variants
-
Toll-like receptor polymorphisms (for example TLR2, TLR4)
Effect
-
Slower fungal recognition
-
Increased colonisation or allergic response
-
Act as risk amplifiers, not causes
Cytokine balance variants
Small genetic differences affecting immune “signal strength”, including:
-
Interleukin-6
-
Interleukin-10
-
Tumour necrosis factor-alpha
These modify:
-
Inflammation intensity
-
Tissue damage vs clearance balance
Allergy-biased (Th2-skewed) immunity
Not a disease, but a recognised immune tendency.
Features:
-
Asthma
-
Eczema
-
Nasal polyps
-
High immunoglobulin E levels
-
Eosinophilia
Strongly associated with:
-
Fungal sensitisation
-
ABPA
-
Difficult-to-control asthma
Impaired mucociliary clearance
A functional immune–mechanical issue.
Seen in:
-
Severe asthma
-
Bronchiectasis
-
Chronic sinus disease
Effect:
-
Aspergillus spores are not physically cleared
-
Prolonged immune exposure
-
Increased colonisation and allergy
Age-related immune change (immunosenescence)
-
Normal reduction in immune speed and coordination with age
-
Particularly relevant to chronic pulmonary aspergillosis
Not a disease, but an important modifier of outcome.
Airway epithelial vulnerability
Subtle weaknesses in:
-
Airway lining integrity
-
Antimicrobial peptide production
-
Local immune signalling
Can increase:
-
Fungal adherence
-
Chronic colonisation
-
Allergic sensitisation
Section 3: Risk stacking – how this works in real life
Aspergillosis rarely results from one single factor.
Instead, several modest risks align:
-
Mild MBL deficiency
-
Severe asthma
-
Corticosteroid exposure
-
Bronchiectasis
-
Age-related immune change
→ Together, they create real disease risk, even though none alone would.
This explains why:
-
Two people with similar scans can behave very differently
-
One patient relapses while another stabilises
-
“Why me?” often has no single answer
Section 4: When clinicians investigate immune causes
Testing is targeted, not routine. It is usually considered when there is:
-
Aspergillosis at a young age
-
Invasive or unusually severe disease
-
Disease without classic risk factors
-
Recurrent infections plus severe asthma or allergy
-
A family history of unusual infections
Section 5: Why identifying (or excluding) immune factors helps
Understanding immune contribution can:
-
Explain disease pattern and behaviour
-
Guide antifungal choice and duration
-
Inform long-term prevention strategies
-
Reduce future lung damage
-
Reassure patients when no immune defect is found
Key take-home messages
-
Aspergillus exposure is universal; immune causes are rare
-
Only ~20–30 inherited immune deficiencies are clearly linked to aspergillosis
-
Modifier-type immune factors are common and usually harmless alone
-
Aspergillosis often reflects risk stacking, not a single diagnosis
-
Understanding patterns matters more than labels
-
Specialist care improves precision and outcomes
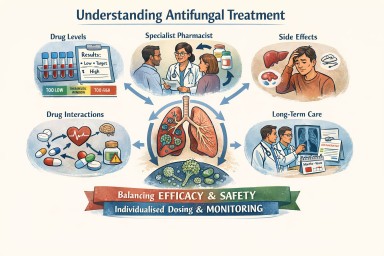
Antifungal Medicines: Dosing, Monitoring, and the Role of Specialist Care
A detailed reference for patients and non-specialist clinicians
1. Why antifungal treatment is different from most medicines
Oral antifungal medicines—especially azole antifungals—are essential for treating long-term fungal diseases such as chronic pulmonary aspergillosis and allergic bronchopulmonary aspergillosis.
They differ from many common medicines because they:
-
Have a narrow margin between effectiveness and toxicity
-
Behave very differently between individuals
-
Are often taken for months or years, not days
-
Interact with many commonly prescribed drugs
For these reasons, antifungal treatment requires individualised dosing, monitoring, and specialist input, rather than a standard fixed dose.
2. What “pharmacokinetics” means (plain language)
Pharmacokinetics describes what the body does to a drug:
-
Absorption – how well the drug enters the bloodstream from the gut
-
Distribution – how effectively it reaches tissues such as the lungs
-
Metabolism – how quickly the liver breaks it down
-
Elimination – how the drug leaves the body
Differences at any of these stages explain why the same dose can be ineffective for one person and toxic for another.
3. Different generations of azole antifungals behave differently
Each generation of azole antifungal was designed to improve effectiveness, but chemical changes also altered how the body handles the drug.
First-generation azoles (older drugs)
Examples
-
Ketoconazole
-
Fluconazole (limited activity against Aspergillus)
Key features
-
Variable absorption
-
Shorter half-life
-
Less reliable lung penetration
Clinical relevance
-
Rarely used now for chronic aspergillosis
Second-generation azoles (mainstay treatment)
Examples
-
Itraconazole
-
Voriconazole
-
Posaconazole
Key features
-
Excellent lung and tissue penetration
-
Highly variable metabolism between people
-
Strong interaction with liver enzymes
Clinical relevance
-
Very effective
-
Blood levels vary widely
-
Dose adjustment and monitoring are often essential
Newer azoles
Example
-
Isavuconazole
Key features
-
More predictable absorption
-
Long, stable half-life
-
Fewer extreme peaks and troughs
Clinical relevance
-
Often better tolerated long-term
-
Monitoring still important, but dosing may be more stable
4. Why the “right dose” matters so much
Too little antifungal
-
Infection not adequately controlled
-
Symptoms persist or worsen
-
Risk of antifungal resistance
-
Fewer future treatment options
Too much antifungal
-
Liver irritation or damage
-
Nausea, appetite loss
-
Neurological or visual side effects
-
Drug accumulation, especially with long-term use
The aim is always the lowest dose that effectively controls the fungus.

5. How clinicians know whether the dose is right
No single test determines this. The correct dose is identified when three elements align:
1️⃣ Blood level testing (therapeutic drug monitoring)
-
Measures how much drug is actually in the bloodstream
-
Helps identify:
-
Under-dosing
-
Target-range dosing
-
Toxic levels
-
2️⃣ Clinical response
-
Symptoms stabilise or improve
-
Fewer flare-ups or complications
-
Better day-to-day function
3️⃣ Safety monitoring
-
Liver and kidney blood tests
-
Review of side effects
-
Ongoing assessment of drug interactions
Only when effectiveness and safety are both acceptable is the dose considered “right”.
6. Why the right dose can change over time
A dose that was correct initially may later need adjustment because of:
-
Weight or body-composition changes
-
Age-related metabolic changes
-
New medications (including antibiotics or steroids)
-
Changes in liver or kidney function
-
Gradual drug accumulation during long-term therapy
Regular review is therefore expected and appropriate.
7. Is it sometimes impossible to find a stable dose?
Yes. For a minority of patients, a perfectly balanced dose cannot be found.
Reasons include:
-
Extremely fast or slow drug metabolism
-
A very narrow safety window
-
Long-term toxicity despite “acceptable” blood levels
-
Unavoidable interacting medications
-
Liver, kidney, or neurological vulnerability
-
Partial or full antifungal resistance
In these cases, the dose that controls the fungus and the dose that causes side effects may overlap.
This reflects biological limits, not treatment failure.
8. What clinicians do when a stable dose cannot be achieved
Options may include:
-
Switching to a different azole with different pharmacokinetics
-
Using modified dosing schedules (split dosing, slower titration)
-
Accepting a lower suppressive dose rather than full eradication
-
Considering non-azole antifungals where appropriate
-
Prioritising symptom control and quality of life
All are intentional, safety-focused decisions.
9. The central role of the specialist pharmacist
Specialist pharmacists are key to safe antifungal care, particularly for long-term azole therapy.
They play a critical role in:
Interpreting drug levels
-
Assessing whether a level is truly low or high
-
Accounting for dose timing and formulation
-
Preventing unnecessary or unsafe dose changes
Managing drug–drug interactions
Azoles interact with many common medicines, including:
-
Steroids and inhalers
-
Heart rhythm drugs
-
Blood thinners
-
Anti-epileptics
-
Pain medications
The specialist pharmacist:
-
Reviews the full medication list
-
Anticipates interactions before harm occurs
-
Advises on adjusting both interacting drugs
Individualising dosing
When standard doses do not work, they help design:
-
Non-standard doses
-
Split dosing schedules
-
Slow titration plans
-
Alternative azoles with different pharmacokinetics
Protecting patients during long-term treatment
They monitor:
-
Trends in liver and kidney tests
-
Signs of cumulative toxicity
-
Whether symptoms may be drug-related rather than disease-related
Coordinating care
They act as a bridge between:
-
Laboratory results
-
Clinical decision-making
-
Patient experience

Their involvement often changes management, not just fine-tunes it.
10. Where antifungal drug level testing is done in the UK
In the UK, antifungal drug level testing is centralised.
-
Blood samples are taken locally
-
Samples are sent to specialist reference laboratories, most commonly the
Mycology Reference Centre Manchester -
Results are returned to the local clinical team for interpretation
Patients managed through specialist services such as the
National Aspergillosis Centre
benefit from integrated expertise in antifungal pharmacology, imaging, and long-term monitoring.
This process is routine and standard for antifungal care.
11. Key reassurance for patients
-
Dose changes are normal and expected
-
Side effects are often biology-driven, not your fault
-
Blood tests make treatment safer, not riskier
-
Switching drugs is a planned strategy, not giving up
12. One-paragraph summary
Antifungal medicines—particularly azole antifungals—have complex and highly variable behaviour in the body, with a narrow balance between effectiveness and toxicity. Safe use requires individualised dosing, therapeutic drug monitoring, symptom review, and long-term safety checks. Specialist pharmacists play a central role in interpreting drug levels, managing interactions, and tailoring treatment. For some patients, a perfectly balanced dose cannot be achieved, and alternative strategies are required. This reflects biological complexity, not failure, and the overarching aim is always effective fungal control with the best possible long-term safety and quality of life.
Airways mucus and aspergillosis
A clear, patient-friendly explainer
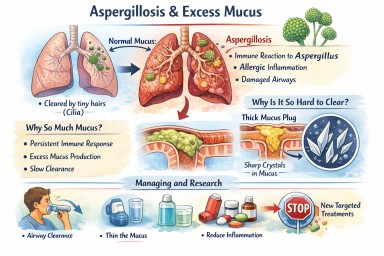
People living with aspergillosis often say that mucus is one of the hardest symptoms to manage — thick sputum, coughing fits, plugs that feel “stuck”, and flare-ups that seem to come out of nowhere. This explainer brings everything together in one place: what mucus is for, why aspergillosis causes so much of it, why it becomes abnormal, and what current and future treatments aim to do.
1. What is airway mucus and why do we need it?
Mucus is normal, healthy, and essential. Everyone produces it all the time.
Its main roles are to:
-
Trap inhaled particles (dust, spores, bacteria, pollution)
-
Protect the airway lining from drying and irritation
-
Support the immune system
-
Clear the lungs, using tiny moving hairs (cilia) that sweep mucus upwards so it can be swallowed or coughed out
(this clearance system is called the mucociliary escalator)
In healthy lungs:
-
Mucus is thin
-
Produced in small amounts
-
Cleared without you noticing it
2. Why aspergillosis causes excessive mucus
In aspergillosis, the lungs are under ongoing stress. Several factors combine:
Persistent immune activation
The immune system keeps reacting to Aspergillus material in the airways. Even when the fungus is controlled, inflammation can persist.
Allergic-type inflammation (especially in ABPA)
Allergic immune responses strongly stimulate mucus-producing cells, leading to:
-
Large volumes of mucus
-
Very sticky or rubbery sputum
Airway damage
Conditions commonly associated with aspergillosis (such as bronchiectasis or long-standing asthma) cause:
-
Widened or damaged airways
-
Poor mucus clearance
-
Pools of mucus that are hard to shift
Slowed clearance
Inflammation and infection impair cilia, so mucus:
-
Moves more slowly
-
Sits in the lungs longer
-
Becomes thicker and harder to clear
➡️ What starts as a protective response becomes a self-perpetuating problem.
3. Why thick mucus causes symptoms
Excess or abnormal mucus can:
-
Block airways → breathlessness and wheeze
-
Trigger coughing → especially overnight or on waking
-
Trap infection → repeated flare-ups
-
Reduce oxygen exchange
-
Increase fatigue and chest discomfort
Many patients describe it as:
“Glue-like”, “stringy”, “rubbery”, or “impossible to move”
4. Mucus plugs and crystals – why some mucus is so hard to clear
Mucus plugs
When mucus becomes very thick, it can:
-
Form plugs that partially or completely block airways
-
Show up on CT scans
-
Worsen breathlessness suddenly
Charcot–Leyden crystals
In allergic and eosinophilic airway disease (including allergic bronchopulmonary aspergillosis):
-
Breakdown products of allergic immune cells can form microscopic crystals
-
These crystals make mucus:
-
Stiffer
-
More irritating
-
Harder to clear
-
Their presence is a sign of ongoing allergic inflammation, not infection alone.
5. Why managing mucus really matters
Mucus is not just an inconvenience. Poor mucus control can:
-
Increase infection risk
-
Drive repeated exacerbations
-
Worsen lung damage over time
-
Reduce quality of life and sleep
-
Increase hospital admissions
For aspergillosis, mucus management is core treatment, not optional.
6. What helps now (current approaches)
A. Thin the mucus
-
Good hydration
-
Nebulised saline (normal or hypertonic)
-
Selected mucolytic medicines (used carefully)
B. Move it out
-
Regular airway clearance physiotherapy
-
Breathing techniques (e.g. active cycle breathing)
-
Oscillating devices (flutter, Acapella, Aerobika)
-
Gentle, regular physical activity where possible
C. Reduce inflammation
-
Inhaled corticosteroids (when appropriate)
-
Oral steroids (used cautiously)
-
Biologic therapies for selected allergic or eosinophilic disease
-
Antifungal treatment when fungal burden is contributing
D. Treat infections early
-
Bacterial infections thicken mucus further
-
Prompt treatment reduces long-term damage
7. What research is doing differently (emerging therapies)
Research is moving beyond simply “loosening mucus”.
1. Reducing mucus production at source
Scientists are developing drugs that aim to:
-
Switch off excessive mucus secretion
-
Preserve normal protective mucus
This targets the mucus-producing cells directly.
2. Blocking the signals that drive over-production
Inflammation sends chemical signals telling airways to make more mucus. New treatments aim to:
-
Calm allergic and immune pathways
-
Prevent expansion of mucus-producing cells
Some current biologic therapies already reduce mucus indirectly; future drugs will be more precise.
3. Changing mucus structure
Instead of thinning everything, researchers are studying ways to:
-
Loosen the internal “mesh” of mucus
-
Prevent dense plugs from forming
-
Restore normal movement by cilia
4. Targeting mucus crystals
In allergic aspergillosis, research is exploring how to:
-
Reduce crystal formation
-
Calm the specific immune responses that create them
5. New inhaled and physical approaches
Early trials are testing:
-
Inhaled therapies designed to mobilise secretions
-
Treatments that improve airflow behind mucus plugs
6. Precision medicine
Future mucus treatments are likely to be:
-
Personalised
-
Based on inflammation type, fungal involvement, airway damage, and immune markers
Two people with aspergillosis may have very different mucus drivers — and need different solutions.
8. What this means for patients today
-
There is no single “anti-mucus cure” yet
-
Promising therapies are in research and early trials
-
Safety and long-term effects must be proven first
For now:
-
Regular airway clearance remains essential
-
Treating inflammation and infection promptly is crucial
-
Understanding why your mucus behaves as it does helps guide treatment
Key messages to remember
-
Mucus is normally protective
-
Aspergillosis turns a helpful system into a problem
-
Thick, sticky mucus reflects ongoing inflammation and airway damage
-
Crystals signal allergic involvement, not just infection
-
Research is moving toward preventing abnormal mucus formation, not just thinning it
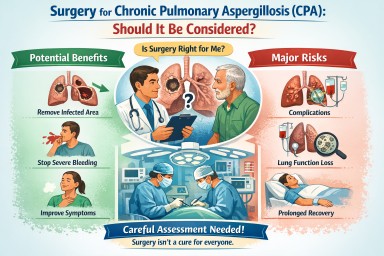
Surgery for Chronic Pulmonary Aspergillosis (CPA): why it is sometimes considered – and often not
For people living with chronic pulmonary aspergillosis (CPA), the idea of surgery can raise difficult questions. Some patients are told surgery might offer a chance of cure; others are advised very firmly against it. Both positions can be correct, depending on the individual situation.
This article explains when surgery may be considered, why it is often avoided, and what “success” or “cure” really means in CPA.
Why is surgery even considered in CPA
CPA usually develops in lungs that are already damaged (for example, by tuberculosis, chronic obstructive pulmonary disease, bronchiectasis, sarcoidosis, or prior infections). Antifungal medicines are therefore the mainstay of treatment.
However, surgery may be considered in a small and carefully selected group of patients, most commonly when:
1. Disease is localised to one area of the lung
If the aspergillus infection is confined to a single cavity or one lobe, and the rest of the lungs are relatively healthy, it may be technically possible to remove the affected area.
2. Recurrent or life-threatening haemoptysis (coughing up blood)
Large-volume or repeated bleeding is one of the strongest reasons surgery is considered. In some cases, surgery is viewed as a way to prevent catastrophic bleeding, rather than to eradicate infection.
3. A simple aspergilloma
Patients with a simple aspergilloma (a single fungal ball in a cavity, minimal surrounding disease, and preserved lung function) are the group most likely to benefit.
4. Failure or intolerance of antifungal therapy
If antifungal drugs cannot be taken long term due to side effects, drug resistance, or lack of response—and the disease remains localised—surgery may be discussed.
Why surgery is often not recommended
Although surgery can sound appealing, CPA surgery is high-risk and not suitable for most patients.
1. CPA is often widespread
Many patients have a disease affecting both lungs or multiple lobes. Removing one area does not treat the remaining infection.
2. Underlying lung reserve is limited
CPA commonly occurs in people with reduced lung function. Removing lung tissue can lead to:
-
Long-term breathlessness
-
Oxygen dependence
-
Reduced quality of life
Even if the operation itself is technically successful.
3. Surgery carries significant risks
Compared with many other lung operations, CPA surgery has higher complication rates, including:
-
Prolonged air leaks
-
Serious infections
-
Bleeding
-
Bronchopleural fistula (abnormal airway–pleural connection)
-
Need for prolonged hospitalisation or intensive care
4. Surgery does not address the underlying vulnerability
CPA reflects an ongoing susceptibility of the lung environment. Removing one fungal focus does not remove the underlying reason aspergillus was able to grow in the first place.
What is the “success rate” of surgery?
Success depends heavily on patient selection and surgical expertise.
In specialist centres:
-
Operative mortality (risk of death around the time of surgery):
Typically reported between 1–5%, but higher in complex diseases. -
Major complication rates:
Often 15–40%, depending on disease extent and lung health. -
Symptom improvement:
Many patients selected for surgery experience reduced haemoptysis and improved local control of disease.
These figures are why surgery is only offered after careful multidisciplinary discussion, usually involving respiratory physicians, infectious disease specialists, thoracic surgeons, and radiologists.
Is surgery a “cure” for CPA?
This is one of the most misunderstood points.
Short answer: sometimes, but often not in the long term
-
In a simple aspergilloma, surgery can be genuinely curative if:
-
The disease is completely removed
-
There is no other active CPA elsewhere
-
The patient’s lungs remain stable
-
-
In chronic cavitary or fibrosing CPA, surgery is rarely a true cure. Instead, it may:
-
Control bleeding
-
Remove a particularly problematic area
-
Reduce fungal burden
-
Even after apparently successful surgery, some patients still require:
-
Long-term antifungal therapy
-
Ongoing monitoring with scans and blood tests
Recurrence of aspergillus infection elsewhere in the lungs can occur months or years later.
Why are many patients managed medically instead
For most people with CPA, long-term antifungal therapy offers:
-
Disease stabilisation
-
Symptom control
-
Lower risk than surgery
While antifungals do not usually “cure” CPA either, they can:
-
Slow or halt progression
-
Reduce inflammation and symptoms
-
Improve quality of life
This is why surgery is best seen as a highly selective tool, not a standard treatment.
How decisions about surgery are made
If surgery is discussed, your team will usually consider:
-
Extent and pattern of CPA on imaging
-
Lung function tests
-
General fitness and other medical conditions
-
History of haemoptysis
-
Response and tolerance to antifungal treatment
-
Your own priorities and acceptable trade-offs
Importantly, being told surgery is not advised does not mean your care is being limited—it usually reflects a judgement that risks outweigh benefits in your specific case.
Key messages for patients
-
Surgery for CPA is uncommon and highly selective
-
It is most useful in localised disease or severe bleeding
-
Complication rates are significant
-
A guaranteed or permanent “cure” is not typical, except in carefully chosen cases
-
Long-term medical management remains the safest and most effective option for most patients
If surgery has been mentioned—or ruled out—in your case, it is reasonable to ask your team:
-
What specific problem would surgery aim to solve for me?
-
What risks apply to my lungs and overall health?
-
Would antifungal treatment still be needed afterwards?
These discussions are an important part of shared decision-making in CPA care.